Fatty Liver and Cholesterol: The Connection Explained

Something feels off — persistent fatigue, fullness in the upper abdomen, a cholesterol panel that keeps coming back wrong despite eating “pretty well.” It is easy to blame stress or age. But these signals sometimes point to something more specific happening inside the liver.
When the liver accumulates excess fat, it rarely does so in isolation. The same metabolic environment that allows fat to build up also disrupts how the body processes cholesterol — and the two problems reinforce each other in ways that standard advice rarely addresses.
The encouraging news: the connection between fatty liver and cholesterol is well understood, and the same lifestyle shifts that improve one tend to move the other in the right direction. Understanding this link is one of the most practical things anyone managing metabolic health can do.
Quick Wins
- A 5–10% reduction in body weight is one of the most evidence-backed steps for improving liver fat
- Replacing refined carbohydrates with fiber-rich whole foods lowers both triglycerides and liver fat simultaneously
- Short movement breaks after meals — even 2–5 minutes of light walking — may meaningfully reduce post-meal glucose and take pressure off the liver
- Monitoring triglycerides (not just LDL) gives a clearer picture of liver-cholesterol stress
What Is the Connection Between Fatty Liver and Cholesterol?
Fatty liver and cholesterol are connected through a shared metabolic root: insulin resistance. When the body becomes less sensitive to insulin, the liver begins accumulating triglycerides — and simultaneously loses its ability to process and export cholesterol efficiently.
The result is a pattern that shows up repeatedly in metabolic blood panels: elevated triglycerides, low HDL (“good cholesterol”), and increased small dense LDL particles. The fatty liver and cholesterol connection is not coincidental — it is mechanistic, driven by the same upstream dysfunction.[1]
This is why triglycerides often rise before people realize the liver is involved. And it is why addressing one condition without the other often produces only partial results.

Understanding Fatty Liver Disease
Fatty liver disease develops when fat accounts for more than 5% of the liver’s total weight. In most cases, alcohol is not involved — the condition is driven by diet, metabolic dysfunction, and genetic factors.
The older term NAFLD (nonalcoholic fatty liver disease) is still widely used and the primary search term most people recognize. Clinically, it has been renamed MASLD — metabolic dysfunction-associated steatotic liver disease — to better reflect what actually drives it.
Simple Steatosis Versus NASH
Not all fatty liver is the same. Simple steatosis means fat is present, but the liver cells themselves are not significantly inflamed or damaged — yet.
NASH (nonalcoholic steatohepatitis) is the more serious stage. It involves active inflammation, hepatocyte damage, and the potential for fibrosis. Research indicates that a meaningful proportion of people with steatohepatitis will develop fibrosis over time — making early identification clinically important.[3]
One pattern that shows up repeatedly in clinical data: people caught at the NASH stage often had no obvious symptoms for years. Fatigue and mild right-side abdominal discomfort are sometimes the only signals — easy to attribute to stress, a busy schedule, or just getting older.
Cholesterol Fundamentals and Liver Function
The liver is not a passive bystander in cholesterol metabolism — it manufactures cholesterol daily, packages it into lipoproteins, and removes excess amounts through bile production.
When the liver is under metabolic stress — from excess fat accumulation, insulin resistance, or chronic inflammation — its ability to regulate cholesterol output becomes compromised. The liver begins overproducing VLDL particles, which drives the characteristic lipid pattern seen so often alongside fatty liver disease.
What LDL and HDL Are Actually Doing
LDL carries cholesterol from the liver outward to tissues. HDL collects excess cholesterol and returns it to the liver for recycling. When the liver is stressed by excess fat, it tends to produce more small, dense LDL particles — the type most associated with cardiovascular risk, even when total LDL cholesterol appears within normal range.[2]
Triglycerides tell a related story. In many people with fatty liver, triglycerides are often elevated — because the same insulin resistance that fills the liver with fat also drives excess VLDL production, flooding the bloodstream with these lipids simultaneously.
This is also why people can feel heavy and tired after meals long before any formal diagnosis is made. The metabolic system is working harder than it should at every meal.
The Mechanisms Driving the Link
Insulin resistance is the first driver. When cells stop responding well to insulin, the liver receives a continuous signal to increase fat production — even when the body does not need more fuel stored.
This excess fat accumulation then creates a second problem: the stored lipids themselves begin generating oxidative stress, damaging liver cells and triggering inflammation. That inflammation does not stay local — it enters circulation and affects blood vessels, metabolic signaling, and cardiovascular risk over time.
Why This Creates a Cycle
The key insight here is that the two conditions feed each other. Fatty liver worsens insulin resistance, which drives more fat into the liver. Elevated triglycerides contribute to more small dense LDL production. And chronic low-grade inflammation — coming from both the liver and fat tissue — makes every part of this worse.
In practice, this means improving insulin sensitivity often improves both lab markers together. That is actually the encouraging part of this picture.
What Can Actually Help
The research here is more encouraging than most people expect. Because fatty liver and cholesterol share a common metabolic root, targeting that root tends to move both markers in the right direction at the same time.
Start With This
The single most accessible first step: short movement breaks after meals. Research shows that light-intensity walking for just 2–5 minutes after eating may significantly reduce postprandial glucose and insulin compared to sitting — a direct way to reduce the metabolic load on the liver after each meal.[5]
Pair that with a protein-forward breakfast — eggs, Greek yogurt, or cottage cheese. Starting the day with protein tends to reduce morning glucose excursions and may help keep insulin lower through the first half of the day.
Add This Next
Triglycerides often respond relatively quickly to dietary change — many people see reductions within 2–4 weeks of consistently cutting back on refined carbohydrates and sweetened beverages.
Liver fat reduction takes longer. Research suggests meaningful improvements in hepatic fat content tend to appear over 8–12 weeks of sustained dietary change and moderate physical activity. That is still a relatively short window for a condition that may have been developing quietly for years.
What to Watch For
The early signals that things are shifting: afternoon energy often stabilizes first. The heavy post-meal fatigue that many people with fatty liver experience tends to lessen — sometimes within the first few weeks — as the metabolic load on the liver begins to ease.
On the lab side: watch triglycerides and the triglyceride-to-HDL ratio alongside LDL. A triglyceride-to-HDL ratio above 3 is a reasonably useful indicator of insulin resistance and hepatic stress — and it often moves before LDL does.

Why This Also Affects Your Heart
One thing that often surprises people: fatty liver disease is not just a liver problem. The same metabolic dysfunction that fills the liver with fat also raises cardiovascular risk — and the connection runs through chronic low-grade inflammation.
When the liver is under sustained metabolic stress, it releases inflammatory signals that circulate throughout the body. C-reactive protein (CRP) — a measurable inflammation marker — is consistently elevated in people with advancing fatty liver, and that same elevation is associated with arterial inflammation and increased cardiovascular event risk.[6]
This is why cardiovascular disease is the leading cause of mortality in people with NAFLD — not liver failure. The two systems are more connected than most people realize, which is also why improving liver health tends to show up across multiple markers at once.
Dietary Choices That Make a Measurable Difference
The Mediterranean dietary pattern has the strongest direct evidence for improving both liver fat and cholesterol profiles among commonly studied eating approaches. It is worth being specific about why — because “eat more vegetables” misses the mechanism.
The combination of olive oil, fatty fish, legumes, and fibrous vegetables works through multiple pathways: reducing the liver’s production of new fat from carbohydrates, lowering triglycerides, and improving insulin sensitivity simultaneously.[8]
One thing worth pushing back on here: many nutrition guides list Mediterranean, DASH, and plant-based diets as roughly equivalent options. For liver fibrosis outcomes specifically, the Mediterranean pattern has the strongest and most direct evidence. The others are reasonable choices — but they are not interchangeable for this indication.
Specific Foods Worth Prioritizing
The foods with the most consistent evidence for liver-cholesterol benefit: extra virgin olive oil, fatty fish (salmon, sardines, mackerel), walnuts, leafy greens, legumes (lentils, chickpeas), and berries.
What tends to drive both liver fat and triglycerides up most consistently: added sugars — particularly fructose from sweetened beverages — and refined carbohydrates that spike insulin repeatedly throughout the day.
| Food Category | Primary Benefit | Examples | Practical Goal |
|---|---|---|---|
| Anti-inflammatory fats | Reduces liver inflammation; improves cholesterol ratios | Extra virgin olive oil, walnuts, fatty fish | Use as primary fat sources daily |
| Fiber-rich vegetables | Slows glucose absorption; feeds gut bacteria that support liver health | Leafy greens, broccoli, zucchini, peppers | Half the plate at most meals |
| Legumes | Soluble fiber lowers LDL; protein supports satiety without spiking insulin | Lentils, chickpeas, black beans | 3–4 servings per week |
| Limit: added sugars | Fructose drives hepatic fat production and elevated triglycerides | Sweetened beverages, fruit juices, packaged snacks | Minimize — especially liquid sugar |
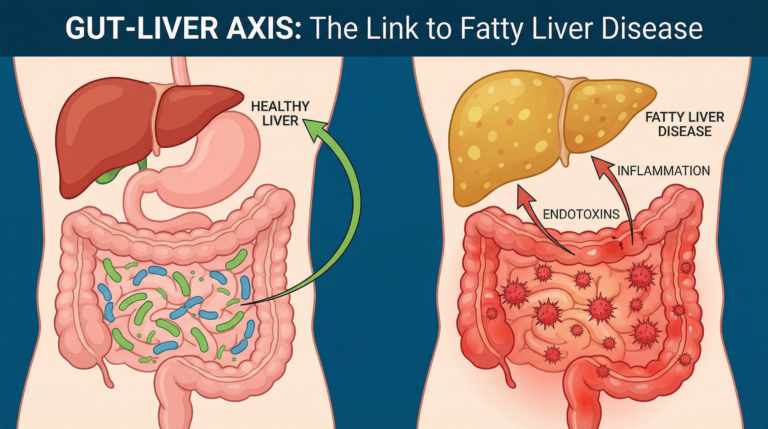
The gut-liver connection is worth understanding more deeply here — the bacteria in the digestive tract directly influence how much inflammatory signaling the liver receives via the portal vein. A fiber-rich diet is one of the most direct ways to support that pathway. More on this in The Gut-Liver Axis and Fatty Liver.
Lifestyle Modifications for Managing Fatty Liver
Weight reduction remains the single most evidence-backed intervention for fatty liver. Even a 5–10% reduction in body weight tends to produce measurable improvements in hepatic fat content and liver enzyme levels.
That 5–10% is not a large number. For someone at 180 lbs, it is 9–18 lbs. The change is achievable — and the liver tends to respond relatively quickly once that direction is established.
Exercise: Type and Timing Both Matter
Both aerobic exercise and resistance training may improve insulin sensitivity — the upstream driver of both fatty liver and cholesterol dysregulation. Aim for roughly 150 minutes of moderate movement per week, which works out to about 20–25 minutes most days.
Short movement breaks after eating deserve specific mention. Light walking for 2–5 minutes after meals tends to reduce postprandial glucose and insulin more effectively than standing or continued sitting — directly reducing the post-meal lipid and glucose load that stresses the liver over time.[5]
What to Track Beyond LDL
Standard cholesterol panels focus on LDL. For fatty liver, triglycerides and the triglyceride-to-HDL ratio are often more informative — they tend to reflect the metabolic environment more directly.
Liver enzymes (ALT and AST) are inexpensive, widely available, and worth requesting specifically if metabolic risk factors are present. Many people with early fatty liver have normal lipid panels but elevated ALT — a detail that often goes unremarked in routine bloodwork. For a full breakdown of what each liver enzyme number actually means, see What Your Liver Enzyme Results Actually Mean.
| Modification | Primary Benefit | Practical Target |
|---|---|---|
| Weight reduction | Reduces hepatic fat; improves liver enzymes | 5–10% of body weight, at a sustainable pace |
| Post-meal movement | Blunts post-meal triglyceride and glucose spikes | 2–5 min light walking immediately after eating |
| Aerobic exercise | Lowers triglycerides; improves insulin sensitivity | 150 min/week (~20–25 min daily) |
| Resistance training | Builds muscle mass to improve glucose uptake | 2–3 sessions per week |
Treatment Options and Medical Interventions
When lifestyle adjustments alone are insufficient, pharmacological options exist — but they address different parts of the problem, and understanding which is which matters.
Statins: What They Do (and What They Don’t)
Statins are the most commonly prescribed medications for elevated LDL cholesterol. They are generally safe for people with fatty liver disease, and research shows that people with NAFLD who received statins had significantly lower cardiovascular event rates than those who did not.[2]
This is where the standard advice tends to oversimplify: statins address LDL and cardiovascular risk, but they do not meaningfully target insulin resistance — the core driver of both fatty liver and the triglyceride/HDL pattern that characterizes metabolic dyslipidemia. Someone on a statin whose diet is high in refined carbohydrates may have controlled LDL but worsening liver fat. The two issues require different tools.
Other Interventions Worth Knowing About
Vitamin E (800 IU/day of RRR α-tocopherol) has demonstrated histological benefit for NASH in people without diabetes — this is one of the few pharmacological interventions referenced in AASLD guidelines for confirmed NASH with advanced fibrosis. It is not a first-line option; discuss with a doctor before supplementing.[3]
Certain diabetes medications — particularly GLP-1 receptor agonists and pioglitazone — improve insulin sensitivity at the liver level and are increasingly being studied for MASLD treatment. For people who also have type 2 diabetes or prediabetes, treating that underlying condition often produces meaningful liver improvements as a downstream effect.
Conclusion
Fatty liver and cholesterol are not two separate problems that happen to coexist — they share a common metabolic origin, and improving one tends to support the other. That is not a small insight. It means that consistent, targeted changes can move multiple markers at once.
This condition develops quietly, often without obvious symptoms. So many people are caught off guard when a doctor mentions elevated liver enzymes or an abnormal lipid pattern. It is not a personal failure — it is a metabolic process, and metabolic processes respond to input.
The changes that matter most are not dramatic: less liquid sugar, more fiber-rich whole foods, movement after meals, gradual weight reduction if needed. Each of these pulls in the same direction. The biology here is genuinely working in your favor — the liver is one of the few organs that can meaningfully recover when the conditions that stressed it are changed.
Frequently Asked Questions
What is the connection between fatty liver and cholesterol?
The fatty liver and cholesterol connection runs through insulin resistance, which is the shared metabolic driver of both conditions. When insulin signaling breaks down, the liver accumulates triglycerides and simultaneously overproduces VLDL particles — raising triglycerides, increasing small dense LDL, and lowering HDL cholesterol. This is why abnormal cholesterol patterns and fatty liver so often appear together on the same blood panel. Addressing insulin resistance through diet and movement tends to improve both conditions at once.
Can you have high cholesterol without having a fatty liver?
Yes, and it happens regularly. Elevated LDL can stem from genetic factors — familial hypercholesterolemia, for example — independent of liver fat accumulation. However, when elevated triglycerides and low HDL appear together alongside high LDL, that combination is more suggestive of the metabolic dyslipidemia associated with fatty liver disease. If elevated cholesterol is accompanied by fatigue, weight gain around the midsection, or elevated liver enzymes (ALT/AST), it is worth asking a doctor to evaluate liver health specifically.
Does lowering cholesterol automatically improve liver health?
Not automatically. Statins lower LDL and reduce cardiovascular risk, and they are generally safe for people with fatty liver disease. But they do not address the insulin resistance or dietary patterns that drive hepatic fat accumulation. Improving the full lipid picture — particularly lowering triglycerides and raising HDL — through dietary change and physical activity tends to benefit the liver more directly than LDL reduction alone. The most effective approach targets both simultaneously.
What foods are most helpful for both fatty liver and cholesterol?
The Mediterranean dietary pattern has the strongest evidence among commonly studied approaches for improving both conditions together. Practically, this means prioritizing extra virgin olive oil, fatty fish like salmon and sardines, leafy greens, broccoli, peppers, lentils, chickpeas, walnuts, and berries. Reducing sweetened beverages and refined carbohydrates tends to lower triglycerides relatively quickly — often within two to four weeks of consistent change. These foods address both liver fat and the cholesterol imbalance driven by metabolic dysfunction.
If I’m not overweight, can I still develop fatty liver?
Yes. This is called lean NAFLD or lean MASLD, and it is more common than previously recognized. The drivers in these cases are typically insulin resistance, a diet high in fructose or refined carbohydrates, and sometimes genetic factors affecting how the liver handles lipids. In parts of Asia, lean NAFLD accounts for nearly a quarter of all cases. Body weight alone is not a reliable indicator of liver health — metabolic markers like triglycerides, fasting insulin, and liver enzymes are more informative than BMI for this purpose.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or treatment plan. TheMetabolicHub.com does not replace professional medical guidance.
References
- Chalasani N, et al. Nonalcoholic Fatty Liver Disease and Metabolic Syndrome. Clin Liver Dis. 2018. PMID: 29128053
- Chatrath H, Vuppalanchi R, Chalasani N. Dyslipidemia in patients with nonalcoholic fatty liver disease. Semin Liver Dis. 2012. PMID: 22418885
- Chalasani N, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guideline by the AASLD, ACG, and AGA. Hepatology. 2012. PMC: PMC3328950
- Two-hit hypothesis framework for NAFLD/NASH progression. Exploration of Digestive Diseases. explorationpub.com
- Buffey AJ, et al. The acute effects of interrupting prolonged sitting with standing and light-intensity walking on cardiometabolic health biomarkers. Sports Medicine. 2022. PMID: 35147898
- TLR expression and systemic inflammation in liver and aortic tissue. PMC. 2022. PMC: PMC9147364
- NAFLD Activity Score methodology and histological grading. PMC. 2017. PMC: PMC5215469
- Estruch R, et al. Primary prevention of cardiovascular disease with a Mediterranean diet (PREDIMED). N Engl J Med. 2018. PMID: 29897866