Fatty Liver Belly Fat: Why the Link Matters
That firm, stubborn weight around the middle can feel frustrating, especially when meals, walking, or workouts already feel more intentional than they used to. This may not be random: the waistline, liver, insulin, and blood sugar often move through the same metabolic system. The encouraging news: fatty liver belly fat can often be approached with small, repeatable habits that support liver health and metabolic flexibility over time.
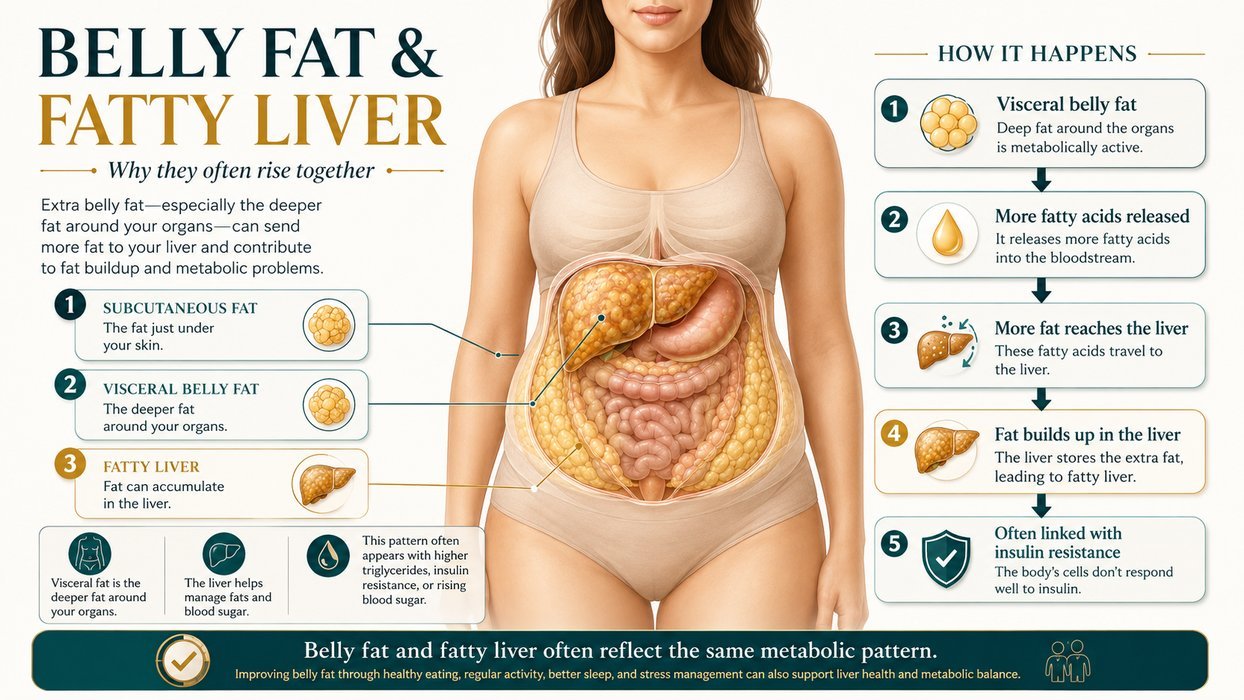
Fatty liver belly fat describes a common pattern where excess liver fat, visceral abdominal fat, and insulin resistance overlap. It is not a separate diagnosis, but it can be a useful way to understand why belly fat sometimes feels harder to shift than weight in other areas.
Quick Win: After one main meal today, take a relaxed 10–15 minute walk. This small habit may help muscles use glucose more efficiently and can support the liver–insulin connection over time.
Fatty liver belly fat: what is the connection?
Fatty liver and stubborn belly fat are often connected through insulin resistance, visceral fat, and the way the liver handles glucose and fats. The liver sits at the center of this system because it helps regulate blood sugar, process fatty acids, and store or release energy.
Fatty liver belly fat is most often a metabolic pattern, not a willpower problem. Many adults begin to notice early changes within a few weeks when meals, walking, strength training, sleep, and alcohol intake become more consistent, while lab and waist changes usually need several weeks to months.
When the liver accumulates excess fat, it is commonly part of a broader condition now called metabolic dysfunction-associated steatotic liver disease, or MASLD. This condition was previously called nonalcoholic fatty liver disease, or NAFLD.[1]
Clinical context: Recent MASLD guidance estimates that global prevalence has risen from about 25% in 2016 to more than 30% today. That does not mean every expanding waistline is fatty liver, but it does explain why this pattern deserves calm, early attention.[2]
Key takeaways
- Fatty liver and belly fat often overlap because both are linked to insulin resistance and visceral fat.
- Visceral fat is metabolically active and can increase fatty acid delivery toward the liver.
- Waist size cannot diagnose liver fat, but it can be a useful clue when combined with labs and risk factors.
- Protein, fiber, unsaturated fats, fewer sugary drinks, and regular movement may support liver and waistline changes.
- Post-meal walking and strength training can support glucose handling even before major scale changes appear.
- Medical follow-up matters because fatty liver can be silent and liver enzymes may not tell the whole story.

Why the liver and waistline often change together
The liver is not a passive storage tank. It receives nutrients from the gut, helps regulate blood glucose, packages fats for transport, and responds closely to insulin.
When energy intake, insulin resistance, alcohol intake, genetics, sleep debt, medications, or low muscle activity add pressure, the liver may store more fat than it can comfortably process. This can happen gradually and often without obvious symptoms.
Mechanism in plain English: Visceral fat can release fatty acids and inflammatory signals toward the liver. At the same time, insulin resistance can make the liver release glucose when the body does not need as much, while fat handling becomes less efficient.
This is why fatty liver belly fat can feel so stubborn. The issue is not only how much body fat exists, but where fat is stored and how the liver, muscle, pancreas, and fat tissue are communicating.
Some people with a larger waist never develop clinically significant fatty liver. Others develop liver fat with a normal body mass index, especially when visceral fat is higher than expected for their size.
Why visceral belly fat matters for liver health
Belly fat includes both subcutaneous fat under the skin and visceral fat deeper around the organs. Visceral fat is more strongly associated with insulin resistance, inflammation, altered blood lipids, and fatty liver risk.[3]
The liver receives blood from the digestive tract through the portal circulation. When visceral fat is metabolically active, more fatty acids and inflammatory signals may reach the liver and add to its workload.
| Pattern | Why It Matters | What It Can and Cannot Tell You |
|---|---|---|
| Expanding waistline | May suggest higher visceral fat, which is linked to metabolic strain. | Useful for tracking trends, but it cannot diagnose liver fat. |
| Elevated fasting glucose | May reflect insulin resistance and altered liver glucose output. | Needs context from A1C, medications, sleep, stress, and meals. |
| High triglycerides | Often travels with insulin resistance and liver fat accumulation. | Can support suspicion, but it is not liver imaging. |
| Low HDL cholesterol | Can appear alongside central obesity and insulin resistance. | Part of a broader metabolic pattern, not a standalone answer. |
Waist size alone cannot diagnose liver fat. It can, however, help guide a better conversation about labs, imaging, alcohol intake, medications, family history, and cardiometabolic risk.
This is also where body mass index can be misleading. For a deeper explanation of normal-weight metabolic risk, see why BMI can miss liver fat risk.
How insulin resistance connects liver fat and abdominal fat
Insulin helps move glucose from the bloodstream into cells and signals the liver about energy storage. When cells become less responsive to insulin, the body may produce more insulin to keep blood sugar in range.
Higher insulin levels can make fat loss feel harder for some people because the body is receiving stronger storage signals. At the same time, the liver may keep producing glucose when it is not needed.
One thing worth pushing back on here: stubborn belly fat is often framed as a simple discipline problem. This is not a personal failure. Food quantity matters, but insulin resistance, sleep debt, stress, alcohol intake, genetics, medications, hormones, and muscle mass can all influence where fat is stored and how easily it changes.
That distinction matters because a shame-based approach rarely builds better health. A metabolic approach focuses on levers that may improve glucose handling, liver fat, and waist measurements gradually.
Which labs and measurements can clarify the pattern?
A clinician may look at several data points together rather than relying on one number. The goal is not to label a person by a waist measurement, but to understand risk and decide what follow-up makes sense.
Fatty liver is often silent. Many people do not feel liver pain or obvious symptoms, and routine liver enzymes may be normal even when fat is present.[4]
| Marker | Why It May Be Discussed | Important Caveat |
|---|---|---|
| ALT and AST | Can suggest liver cell stress when elevated. | Normal values do not fully rule out liver fat or fibrosis risk. |
| Triglycerides | Often rise with insulin resistance and excess liver fat. | Meal timing, alcohol, genetics, and medications can affect results. |
| Fasting glucose and A1C | Help assess glucose regulation and diabetes risk. | A1C can be affected by anemia, kidney disease, and other factors. |
| Waist measurement | A practical way to track abdominal fat trends. | It does not show whether fat is inside or outside the liver. |
| Imaging or fibrosis tools | May help estimate liver fat or scarring risk. | Choice of test depends on risk profile and clinician judgment. |
Clinical guidelines emphasize risk stratification because the main concern is not only liver fat itself. The bigger question is whether there is inflammation, fibrosis risk, diabetes risk, or cardiovascular risk that needs closer attention.[5]
What not to overinterpret
A single waist measurement, a single liver enzyme result, or a single week of scale change rarely tells the full story. Metabolic health is better understood through patterns over time.
A person can lose water weight without improving liver fat. Another person may see better glucose, triglycerides, or fitness before the scale changes much.
It is also possible for exercise to support liver fat and metabolic markers even when weight loss is modest. That is one reason waist, labs, strength, walking consistency, sleep, and food quality can all matter.
The most helpful question is not “Which number proves progress today?” A better question is “Which two or three signals are moving in the right direction over the next month?”
Fatty liver belly fat nutrition habits that may help
The most useful eating pattern is usually the one that improves consistency, protein intake, fiber intake, and overall energy balance without feeling punishing. For MASLD, clinical guidance commonly emphasizes weight management, limiting added sugars, reducing refined starches, and improving diet quality.[5]
Build meals around protein and fiber
Protein helps preserve lean mass during fat loss and may support fullness. Fiber-rich foods slow digestion, support gut health, and may help reduce post-meal glucose spikes.
A balanced plate could include eggs, fish, tofu, Greek yogurt, poultry, beans, lentils, or tempeh alongside vegetables and minimally processed carbohydrates. This does not require perfection.
Reduce liquid sugar and frequent refined snacks
Sugary drinks are easy to overconsume because they do not create the same fullness as whole foods. Frequent sweetened beverages, desserts, and refined snacks can add energy while making glucose control more difficult.
This does not mean carbohydrates are the enemy. Oats, beans, fruit, potatoes, and whole grains can fit well when portions, protein, fiber, and activity are aligned.

Choose fats that support cardiometabolic health
Fat quality matters. Olive oil, nuts, seeds, avocado, and oily fish often fit into liver-supportive patterns, while frequent large portions of fried foods and processed meats may be less helpful.
A Mediterranean-style pattern is commonly used in metabolic health guidance because it emphasizes minimally processed foods, unsaturated fats, plants, legumes, and seafood. For a deeper next step, explore better fats for fatty liver and how they fit into everyday meals.[6]
Movement strategies for liver fat and waistline support
Exercise supports metabolic health even before major changes appear on the scale. Regular physical activity may help reduce liver fat, improve insulin sensitivity, and support blood pressure, lipids, and glucose regulation.[7]
The best starting point is often walking because it is accessible, scalable, and gentle on recovery. A post-meal walk may be especially useful because working muscles can use some circulating glucose.[8]
Strength training matters more than many people think
Muscle is a major site for glucose disposal. Building or maintaining muscle can improve the body’s capacity to handle carbohydrates and may support long-term weight management.
Two or three simple strength sessions per week can be enough to start. Squats to a chair, wall push-ups, resistance band rows, step-ups, and hip hinges can all be adapted to current ability.
Cardio does not have to be punishing
Moderate-intensity aerobic exercise can support liver and metabolic health. The right intensity usually feels like breathing is elevated, but conversation is still possible.
For people who already train hard, recovery may be the missing variable. Poor sleep and chronic stress can make appetite, cravings, and glucose control more difficult.
Alcohol, sleep, medications, and other overlooked variables
Food and movement matter, but they are not the whole story. Alcohol intake, sleep quality, stress load, menopause transition, thyroid issues, certain medications, and untreated sleep apnea can all influence liver fat, hunger, glucose, and waist patterns.
Alcohol deserves special attention because liver fat can occur with or without heavy alcohol intake. Anyone with abnormal liver enzymes, known liver fat, or rising metabolic risk should ask a clinician what level of alcohol intake is appropriate.
Sleep is another quiet driver. Short sleep and irregular sleep timing can make cravings, glucose regulation, and appetite harder to manage, even when food choices are improving.
Medication review can also be important. Some medications affect weight, insulin sensitivity, appetite, lipids, or liver enzymes, and changes should always be discussed with the prescribing clinician.
What realistic progress can look like
Progress with fatty liver belly fat is usually measured in weeks and months, not days. Early signs often include steadier energy, fewer intense cravings, improved digestion regularity, or better post-meal comfort.
Measurable changes may show up as a smaller waist measurement, improved fasting glucose, lower triglycerides, improved liver enzymes, or better fitness. These changes vary by person and should be interpreted with clinical context.
Guidelines suggest that weight loss can reduce liver fat, and greater weight loss may be associated with broader improvement in liver inflammation or scarring risk. The exact target should be individualized, especially for people with diabetes, eating disorder history, pregnancy, chronic illness, or medication needs.[1]
Exercise research also suggests that liver-fat-related improvements may be more noticeable when training is sustained for longer than three months. That does not make the first few weeks meaningless; it simply sets a more realistic expectation.[7]

A simple 7-day reset for metabolic momentum
This plan is not a treatment protocol. It is a low-pressure structure that may help adults begin improving habits connected to liver fat, insulin resistance, and stubborn abdominal weight.
- Start each day with protein. Choose a breakfast that includes protein and fiber, such as eggs with vegetables, Greek yogurt with berries, or tofu scramble with beans.
- Walk after one meal. Aim for 10–15 minutes at an easy pace after lunch or dinner.
- Replace sweet drinks most days. Use water, sparkling water, unsweetened tea, or coffee without added sugar.
- Add vegetables twice daily. Frozen, roasted, raw, or soup-based vegetables all count.
- Strength train twice. Do 20–30 minutes of beginner-friendly resistance work with body weight, bands, or weights.
- Set a sleep anchor. Keep one consistent wake time or bedtime for the week.
- Plan one lab conversation. If liver fat, glucose, or abdominal weight is a concern, ask a clinician which tests or imaging may be appropriate.
Many people notice the first meaningful changes as steadier hunger, fewer energy dips, or better post-meal comfort. Waist and lab changes usually need more repetition, often several weeks to months.
For the next 2–4 weeks, choose only two tracking points. A waist measurement and a simple habit score, such as post-meal walks completed, can be more useful than checking every possible metric.
Frequently Asked Questions
What is the connection between fatty liver belly fat and metabolism?
Fatty liver belly fat usually points to the overlap between liver fat, visceral fat, and insulin resistance. Visceral fat can send fatty acids and inflammatory signals toward the liver, while insulin resistance can make glucose and fat handling less efficient. This pattern is common in metabolic health concerns, but it needs proper medical evaluation rather than self-diagnosis.
Can someone have fatty liver without looking overweight?
Yes, fatty liver can occur in people who do not appear overweight. Body composition, genetics, insulin resistance, alcohol intake, medications, diet quality, and visceral fat distribution can all play a role. This is one reason lab work and clinical assessment matter more than appearance alone.
Does losing belly fat always mean liver fat is improving?
A smaller waist can be an encouraging sign, especially when it happens alongside better energy, glucose markers, triglycerides, or liver enzymes. However, waist change alone cannot confirm what is happening inside the liver. Imaging, lab trends, and clinician-guided risk assessment may be needed for a clearer picture.
Which foods are most important to reduce for fatty liver risk?
Many adults benefit from reducing sugary drinks, frequent desserts, refined snack foods, and large portions of highly processed meals. It may also help to limit alcohol, especially when liver fat or abnormal liver enzymes are already present. A clinician can give more specific guidance based on labs, medications, and personal health history.
How long does it take to notice changes in waist size or liver markers?
Some people notice steadier energy or fewer cravings within a few weeks of consistent meals, walking, and sleep routines. Waist size and lab markers often need more time, commonly several weeks to months. Exercise-related liver fat changes may be more meaningful when training is sustained for longer than three months.
Conclusion
The connection between fatty liver and stubborn belly fat is not about blame. It is about understanding that the liver, waistline, insulin, muscles, and daily habits are part of the same metabolic conversation.
Fatty liver belly fat may improve as part of a broader shift toward steadier blood sugar, better food quality, more muscle activity, and more consistent recovery. The most useful next step is small enough to repeat and clear enough to measure.
A calmer waistline often starts with calmer inputs: protein-rich meals, fewer liquid sugars, regular walking, strength work, and medical follow-up when the signs point beyond ordinary weight gain.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or treatment plan. TheMetabolicHub.com does not replace professional medical guidance.
References
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023. PMID: 36727674
- Tacke F, Horn P, Wai-Sun Wong V, et al. EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease. Journal of Hepatology. 2024. PMID: 38851997
- Hanlon CL, Yuan L. Nonalcoholic fatty liver disease: The role of visceral adipose tissue. Clinical Liver Disease. 2022. PMC8958250
- National Institute of Diabetes and Digestive and Kidney Diseases. Symptoms & Causes of NAFLD & NASH. NIDDK
- Cusi K, Isaacs S, Barb D, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease. Endocrine Practice. 2022. PMID: 35569886
- Xiong Y, et al. Effects of Mediterranean diet and low-fat diet on liver enzymes and liver fat content in patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis. 2024. PMID: 39076035
- Nam H, Yoo JJ, Cho Y, et al. Effect of exercise-based interventions in nonalcoholic fatty liver disease: A systematic review with meta-analysis. Digestive and Liver Disease. 2023. PMID: 36653265
- Engeroff T, Groneberg DA, Wilke J. After Dinner Rest a While, After Supper Walk a Mile? A systematic review with meta-analysis on the acute postprandial glycemic response to exercise before and after meal ingestion. Sports Medicine. 2023. PMID: 36715875





