The Link Between Fatty Liver and Sleep Apnea

Waking up exhausted after enough hours in bed can feel confusing, especially when cravings, weight, blood sugar, or liver enzymes also feel harder to manage. This may not be random. The encouraging news: fatty liver and sleep apnea can be understood together, which makes the next steps more specific and less blame-based.
Quick Win: For the next 7 nights, track loud snoring, dry mouth, morning headaches, nighttime waking, bathroom trips, and daytime sleepiness in a simple phone note. Bring that pattern to a healthcare provider if symptoms happen often.
How are fatty liver and sleep apnea connected?
Fatty liver and sleep apnea are often connected through overlapping metabolic pathways, especially insulin resistance, intermittent oxygen drops, inflammation, disrupted sleep, and excess liver fat. The relationship is not the same for everyone, but the overlap is clinically important.
In many adults, fatty liver and sleep apnea can reinforce the same metabolic strain from different directions. Sleep apnea may stress oxygen regulation and recovery overnight, while fatty liver often reflects metabolic dysfunction that is also active during the day.[1]
A realistic timeline is measured in weeks to months, not days. Many people notice earlier changes in morning alertness, cravings, or daytime energy before liver enzymes, A1C, or imaging markers shift.
Key takeaways
- Fatty liver is now often described as metabolic dysfunction-associated steatotic liver disease, or MASLD, when cardiometabolic risk factors are present.
- Obstructive sleep apnea can cause repeated airway narrowing, oxygen dips, and brief arousals during sleep.
- Insulin resistance is one of the strongest bridges between liver fat, blood sugar changes, and sleep apnea risk.
- Sleep apnea treatment is more specific than general sleep hygiene; diagnosis usually requires a sleep study.
- This is not a personal failure. Both conditions are shaped by biology, sleep, hormones, anatomy, environment, and daily habits.
What shared metabolic roots link the two?
Fatty liver and sleep apnea often appear alongside the same metabolic pattern. This may include higher fasting glucose, elevated triglycerides, central weight gain, high blood pressure, prediabetes, type 2 diabetes, or reduced insulin sensitivity.
The liver helps regulate glucose storage, fat processing, cholesterol balance, and energy availability. When insulin resistance develops, the liver may keep releasing glucose even when the body already has enough fuel.
At the same time, more fatty acids may flow toward the liver. Over time, this can contribute to liver fat accumulation, especially when poor sleep, alcohol intake, low activity, genetics, or certain medications add pressure.
| Shared Factor | How It May Matter |
|---|---|
| Insulin resistance | May increase liver fat storage and make glucose regulation less stable. |
| Visceral fat | May affect airway pressure and increase fatty acid delivery to the liver. |
| Sleep fragmentation | May influence appetite, stress hormones, daytime energy, and consistency with habits. |
| Intermittent low oxygen | May increase oxidative stress and inflammatory signaling that can affect liver health. |
Sleep apnea can deepen the cycle by making daytime changes harder to sustain. Poor sleep may increase hunger, reduce motivation to move, and make glucose patterns feel less predictable.
For a closer look at the metabolic side of this connection, see how sleep may affect insulin resistance.

How can low oxygen during sleep affect the liver?
One key mechanism in obstructive sleep apnea is intermittent hypoxia. This means oxygen levels repeatedly dip and recover during sleep, often without the person fully remembering each awakening.
The liver stays metabolically active overnight. It helps regulate glucose, fat metabolism, and inflammatory signaling, so repeated oxygen stress may influence how liver cells respond to metabolic pressure.
Research links obstructive sleep apnea with NAFLD and MASLD patterns, including liver enzyme changes, oxidative stress, and more advanced fatty liver features in some people.[3]
The relationship is complex. Not everyone with sleep apnea develops fatty liver, and not everyone with fatty liver has sleep apnea.
Mechanism Box: Repeated airway narrowing may lower oxygen, trigger brief arousals, activate stress signaling, and increase inflammatory pathways. Over time, these signals may interact with insulin resistance and liver fat storage.
Most guides skip this, but it matters: fatty liver is not only a “food problem,” and sleep apnea is not only a “snoring problem.” Both can reflect a metabolic environment where oxygen, insulin, inflammation, and recovery interact night after night.
Why does insulin resistance matter?
Insulin resistance is one of the clearest bridges between fatty liver and sleep apnea. When cells respond less effectively to insulin, the body may need more insulin to keep blood sugar in range.
Higher insulin levels may encourage the liver to store more fat. They may also make it harder to access stored fuel between meals, which can show up as cravings, energy dips, or difficulty with weight management.
Sleep apnea may add another layer by activating the stress response. Repeated arousals and oxygen drops can increase sympathetic nervous system activity, which may make glucose regulation less stable in some adults.[4]
Why weight is not the whole story
Body weight can influence both conditions, but it is not the only factor. Some people with sleep apnea do not have obesity, and some people with fatty liver have a body mass index in the “normal” range.
Neck anatomy, airway structure, alcohol intake, sedating medications, nasal obstruction, genetics, menopause status, and sleep position may affect sleep apnea risk. Liver fat can also be influenced by diet quality, medications, activity, alcohol, genetics, and insulin sensitivity.
A narrow “just lose weight” message can leave people feeling blamed and under-supported. A better approach is to identify modifiable drivers and improve the full metabolic environment step by step.
What signs suggest sleep apnea may be involved?
Sleep apnea can be easy to miss because many people do not remember waking up. A bed partner may notice loud snoring or breathing pauses before the person experiencing them does.
Possible signs include loud snoring, choking or gasping during sleep, morning headaches, dry mouth on waking, frequent nighttime urination, daytime sleepiness, low concentration, irritability, and feeling unrefreshed after a full night in bed.[2]
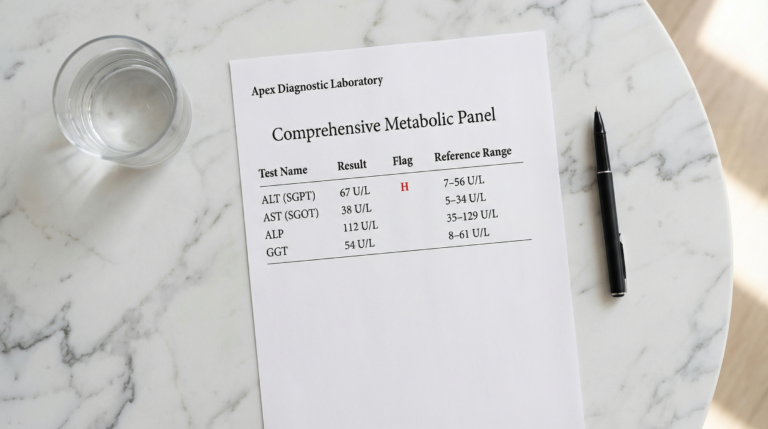
In the context of fatty liver, sleep apnea deserves extra attention when liver enzymes stay elevated, fasting glucose trends upward, blood pressure is higher, or fatigue persists despite nutrition and movement changes.
Clinical context: Reviews suggest obstructive sleep apnea and fatty liver disease are associated even after accounting for some shared risk factors, although individual evaluation still matters.[7]
What to ask your healthcare provider
- Could sleep apnea be contributing to fatigue, glucose changes, or fatty liver risk?
- Would a home sleep apnea test or in-lab sleep study be appropriate?
- Should ALT, AST, A1C, fasting glucose, lipids, or fibrosis risk be monitored?
- Could alcohol, medications, nasal congestion, or sleep position be affecting sleep quality?
- Would CPAP, an oral appliance, positional therapy, or another treatment fit this situation?

What can support progress safely?
Progress usually comes from addressing both nighttime breathing and daytime metabolic habits. The goal is not perfection; it is reducing repeated stress signals that keep the liver and nervous system working harder.
For confirmed obstructive sleep apnea, treatment may include positive airway pressure therapy, oral appliances, positional therapy, weight management support, surgery in selected cases, or another clinician-guided approach.[6]
For fatty liver, evidence-based foundations include regular physical activity, improved diet quality, reduced alcohol exposure, weight reduction when appropriate, and management of blood sugar, blood pressure, cholesterol, and triglycerides.[5]
Nutrition does not need to be extreme. A practical next step is building a MASLD-friendly eating pattern with protein, fiber-rich carbohydrates, unsaturated fats, and fewer sugar-sweetened drinks.
What changes first?
Many people notice earlier shifts in morning alertness, cravings, workout consistency, or afternoon energy. Liver-related lab or imaging changes usually require repeated habits over months.
Useful markers may include waist circumference, blood pressure, sleepiness scores, fasting glucose, A1C, triglycerides, ALT, AST, and non-invasive fibrosis tools when recommended by a clinician.
Nutrition patterns that may support liver and sleep health
A Mediterranean-style pattern may be a flexible fit for many adults. It can include vegetables, legumes, fruit, fish, olive oil, nuts, whole grains, and practical protein choices.
Evening choices can also matter. Large late meals and alcohol close to bedtime may worsen reflux, airway relaxation, snoring, or fragmented sleep in some people.
Movement that supports insulin sensitivity
Physical activity may help improve insulin sensitivity, liver fat regulation, and sleep quality. A balanced routine can include walking, resistance training, and gentle movement after meals.
A 10- to 20-minute walk after dinner is often more realistic than an intense late workout. It may support post-meal glucose handling without overstimulating the body before bed.
A practical 2-week metabolic sleep plan
This plan is educational and should be adapted with a healthcare provider, especially for anyone with diagnosed sleep apnea, diabetes, liver disease, pregnancy, cardiovascular disease, or medication changes.
- Track symptoms for 7 nights. Note snoring, awakenings, morning headaches, dry mouth, daytime sleepiness, and alcohol timing.
- Set a steady wake time. Keep wake time consistent most days, even if bedtime varies slightly.
- Move after dinner. Add a gentle 10-minute walk after the evening meal on at least 5 days.
- Build a protein-forward breakfast. Include protein, fiber, and minimally processed carbohydrates to support steadier appetite.
- Reduce late alcohol and heavy meals. Avoid using alcohol as a sleep aid, especially close to bedtime.
- Book a medical conversation. Bring symptom notes and ask whether sleep apnea screening is appropriate.
The most important shift is moving from guessing to measuring. When sleep, glucose, liver markers, and symptoms are reviewed together, the path forward becomes more specific.
Frequently asked questions
Are fatty liver and sleep apnea directly connected?
Fatty liver and sleep apnea are commonly connected through insulin resistance, metabolic dysfunction, inflammation, and repeated oxygen drops during sleep. Research suggests sleep apnea may contribute to liver stress in some people, especially when metabolic risk factors are also present. The connection is not identical for everyone. A clinician may consider both liver markers and sleep symptoms when building a care plan.
Can treating sleep apnea improve fatty liver?
Treating sleep apnea may support better oxygen stability, sleep quality, daytime energy, and metabolic regulation. Some studies suggest potential liver-related benefits, but results vary. Sleep apnea treatment should not be viewed as a stand-alone fatty liver strategy. Nutrition, movement, alcohol intake, weight management when appropriate, and medical monitoring still matter.
Does snoring mean someone has sleep apnea?
Snoring can be a sign of sleep apnea, but it does not confirm the diagnosis by itself. More concerning signs include witnessed breathing pauses, choking or gasping, morning headaches, daytime sleepiness, and high blood pressure. Some people with sleep apnea do not notice obvious symptoms. A sleep study is usually needed to diagnose obstructive sleep apnea accurately.
Can fatty liver happen in people who are not overweight?
Yes, fatty liver can occur in people who are not classified as overweight. Genetics, insulin resistance, visceral fat distribution, diet quality, alcohol intake, medications, and physical inactivity may all contribute. This is why liver health should not be judged by body size alone. Blood tests, imaging, and clinical context give a more complete picture.
What should someone do first if they suspect both conditions?
A practical first step is to document sleep symptoms, energy patterns, blood pressure readings if available, and recent liver or glucose labs. Bring this information to a healthcare provider and ask whether sleep apnea testing and metabolic liver risk assessment are appropriate. Avoid starting supplements or stopping prescribed medication without professional guidance. Small lifestyle steps can begin right away, but diagnosis and treatment decisions should be individualized.
Conclusion
The link between fatty liver and sleep apnea is not about one single cause. It is about the way breathing, oxygen, insulin resistance, liver fat, and recovery can interact night after night.
For anyone managing fatigue, elevated liver enzymes, prediabetes, cravings, or stubborn metabolic symptoms, sleep deserves a real place in the conversation.
Start with symptom tracking, ask about sleep apnea screening when signs fit, and build steady habits that support the liver, blood sugar, and sleep quality together.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or treatment plan. TheMetabolicHub.com does not replace professional medical guidance.
References
- European Association for the Study of the Liver, European Association for the Study of Diabetes, and European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease. J Hepatol. 2024. PMID: 38851997
- National Heart, Lung, and Blood Institute. Sleep Apnea. NHLBI
- Mesarwi OA, Loomba R, Malhotra A. Obstructive Sleep Apnea, Hypoxia, and Nonalcoholic Fatty Liver Disease. Am J Respir Crit Care Med. 2019. PMID: 30422676
- Murphy AM, Thomas A, Crinion SJ, Kent BD, Tambuwala MM, Fabre A, et al. Intermittent hypoxia in obstructive sleep apnoea mediates insulin resistance through adipose tissue inflammation. Eur Respir J. 2017. PMID: 28424360
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023. PMID: 36727674
- Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2019. PMID: 30736887
- Umbro I, Fabiani V, Fabiani M, Angelico F, Del Ben M. Association between non-alcoholic fatty liver disease and obstructive sleep apnea. World J Gastroenterol. 2020. PMC7265151