Why Lean People Can Still Get Fatty Liver (TOFI Explained)
You may eat fairly well, stay the same clothing size for years, and still feel blindsided when bloodwork or imaging suggests fat in the liver. This may not be random or a sign that you have “missed something obvious.” The encouraging news: lean fatty liver can often be understood through body composition, insulin sensitivity, muscle, and daily metabolic patterns rather than weight alone.
Quick Win: This week, take a 10–15 minute easy walk after your largest carbohydrate-containing meal on at least four days. For most adults, this is a simple, low-risk way to support healthier post-meal blood sugar handling.
Why can lean fatty liver happen?
Lean fatty liver can happen when fat accumulates inside liver cells despite a normal BMI or slim appearance. Common drivers include visceral fat, insulin resistance, low muscle mass, genetics, alcohol exposure, certain medications, and other metabolic stressors.[1]
In lean fatty liver, body weight does not tell the full story. The more useful question is where fat is stored, how well muscle uses glucose, and whether the liver is being asked to handle more energy than it can process comfortably.
Some people notice early lifestyle-related signals within several weeks, such as steadier energy or fewer post-meal crashes. Measurable changes in triglycerides, liver enzymes, imaging, or fibrosis risk often require longer follow-up with a qualified healthcare provider.
Key takeaways
- Lean fatty liver is possible because BMI does not measure liver fat, visceral fat, or muscle quality.
- TOFI means “thin outside, fat inside,” a pattern where internal fat can be higher than appearance suggests.
- Insulin resistance can occur without obvious weight gain and may increase liver fat production.
- Low muscle mass may reduce the body’s glucose storage capacity.
- The goal is usually metabolic improvement, not aggressive weight loss.
Important context: Studies suggest a meaningful share of fatty liver cases occur in people who are not living with obesity. This is one reason liver enzymes, triglycerides, waist measures, glucose markers, and imaging matter alongside BMI.[3]
What does TOFI mean?
TOFI stands for “thin outside, fat inside.” It describes a person who may look slim but carries more visceral fat or ectopic fat than expected.
Visceral fat sits deeper in the abdomen around organs. Ectopic fat means fat stored in places where larger amounts are not usually meant to accumulate, such as the liver, pancreas, or muscle.
Why TOFI matters for liver health
Visceral and ectopic fat are more metabolically active than fat stored under the skin. They are associated with insulin resistance, blood lipid changes, inflammation, and higher cardiometabolic risk, even when weight looks reassuring.[3]
This is not a personal failure. It is a body-distribution pattern that can be missed when health is judged mainly by the scale.
Why BMI can miss the picture
BMI compares weight with height. It does not measure waist size, liver fat, muscle mass, fitness, ethnicity-related risk patterns, or how fat is distributed.
Two people can have the same BMI and very different metabolic profiles. One may have more muscle and less visceral fat, while another may have lower muscle mass, higher liver fat, and higher fasting insulin.
| Measure | What it can show | What it can miss |
|---|---|---|
| BMI | General weight category | Visceral fat, liver fat, muscle mass, fat distribution |
| Waist size | A clue about abdominal fat | Liver fat severity and fibrosis risk |
| Blood tests | Liver enzymes, glucose, triglycerides, A1C, lipid patterns | Some people have fatty liver with normal enzymes |
| Imaging | Evidence of liver fat or stiffness, depending on the test | Daily lifestyle drivers unless interpreted with history |
The mechanism: how liver fat builds up in lean adults
Mechanism in plain English: The liver receives energy from food, stored fat, and newly made fat from excess carbohydrate or calorie intake. When insulin signaling, muscle storage, alcohol exposure, genetics, and visceral fat pressure overlap, more fat may stay in the liver than the liver can export or burn.
Insulin helps move glucose out of the bloodstream and into cells. When muscle and liver cells become less responsive to insulin, the body may produce more insulin to keep blood sugar in range.
Higher insulin exposure may encourage the liver to make and store more fat, especially when paired with frequent refined carbohydrates, sugary drinks, poor sleep, low activity, or alcohol intake.[1]
For readers who notice fatigue, cravings, or post-meal crashes alongside liver concerns, it may be useful to understand the early clues of insulin resistance. These patterns can appear before fasting glucose looks clearly abnormal.

What causes lean fatty liver at a normal weight?
Lean fatty liver usually develops from several overlapping factors rather than one single cause. The common pattern is not simply “too much body weight,” but a mismatch between liver fat handling, insulin signaling, muscle storage, genetics, and lifestyle load.
Low muscle mass can reduce glucose storage space
Muscle is one of the body’s major places to store and use glucose. When muscle mass or muscle function is low, more incoming energy may be handled by the liver instead.
Lean fatty liver has been discussed alongside sarcopenia, a term for low muscle mass and function. Research suggests the relationship may work both ways: liver fat and inflammation may affect muscle, while low muscle may make ectopic fat storage more likely.[4]
Visceral fat can be present even when the body looks lean
Some people store more fat deep in the abdomen rather than under the skin. This can create a TOFI pattern, where external leanness hides internal fat accumulation.
Visceral fat releases fatty acids and inflammatory signals that can reach the liver through portal circulation. Over time, this may contribute to liver fat, triglyceride changes, and impaired metabolic flexibility.
Most guides skip this, but it matters: the common assumption is that less visible fat always means lower metabolic risk. That is partly true for many people, but it misses internal fat distribution, muscle mass, and liver fat. Practically, this means waist-to-height ratio, fitness, labs, sleep, and imaging may tell a more useful story than mirror checks.
Genetics and ethnicity can influence risk
Some people are more prone to liver fat because of inherited differences in how the liver stores and exports fat. Variants affecting liver lipid handling, including PNPLA3, have been associated with fatty liver risk in lean individuals.[5]
Risk can also vary by ancestry and ethnicity. Some populations may develop metabolic complications at lower BMI ranges, which is one reason weight categories should not be treated as the full assessment.
Alcohol, medications, and medical conditions still matter
Fat in the liver is not always driven by the same cause. Alcohol intake, certain medications, viral hepatitis, endocrine conditions, rapid weight changes, and rare lipid disorders may all need to be considered.
Current liver guidance emphasizes assessing alcohol use and cardiometabolic risk factors rather than assuming body size explains the full picture. For lean adults, careful evaluation can help avoid missing less obvious contributors.[6]
How can lean fatty liver show up if weight looks normal?
Many people with fatty liver have no clear symptoms. Others notice vague patterns such as low energy, abdominal fullness, poor exercise recovery, sleepiness after meals, or blood sugar swings.
These symptoms are not specific enough to diagnose liver fat. Lean fatty liver is often found during routine bloodwork or imaging done for another reason.
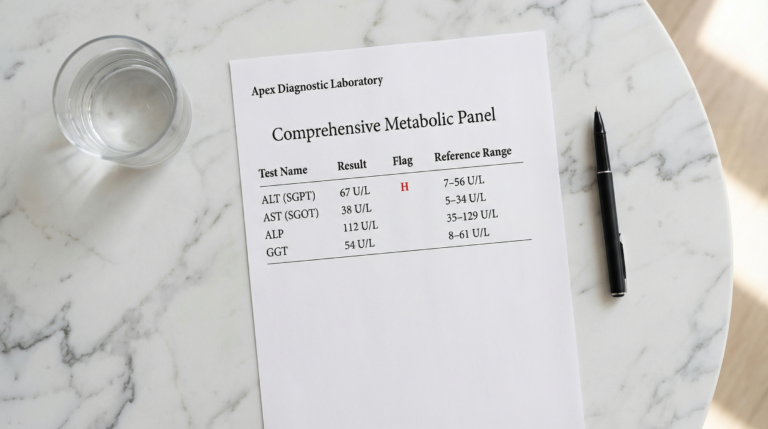
Clues worth discussing with a healthcare provider
- Fatty liver noted on ultrasound, CT, MRI, or FibroScan
- Elevated ALT, AST, GGT, triglycerides, fasting glucose, or A1C
- Normal BMI but increased waist-to-height ratio
- Family history of type 2 diabetes, fatty liver, or early heart disease
- Low muscle mass, low activity, or long periods of sitting
- Regular alcohol intake, even if weight is normal
Clinicians may use non-invasive tools to estimate liver fat and fibrosis risk. These can include blood-based scores, elastography, or imaging, depending on the situation and local availability.[6]
How to support liver fat reduction without chasing weight loss
For lean adults, the goal is usually not aggressive weight loss. The more useful target is better metabolic health: improved insulin sensitivity, lower visceral fat, stronger muscle, steadier blood sugar, and less liver fat over time.
Build meals around protein, fiber, and minimally processed foods
A helpful plate starts with protein, high-fiber plants, and mostly minimally processed carbohydrates. This supports fullness, muscle maintenance, and a slower glucose rise after meals.
Examples include eggs with vegetables, Greek yogurt with berries and nuts, lentil bowls, fish with potatoes and salad, tofu stir-fry, or chicken with beans and roasted vegetables.
Reducing sugar-sweetened drinks and frequent refined snacks may be especially useful. Liquid sugar and highly refined carbohydrates can deliver energy quickly to the liver, particularly when activity is low.
Use resistance training to improve metabolic storage
Strength training helps build or preserve muscle, which may improve the body’s ability to store and use glucose. This can matter even when body weight changes very little.
A practical starting point is two to three full-body sessions per week. Squats, hinges, rows, presses, carries, and step-ups can all be adapted to different fitness levels.
Add easy movement after meals
Post-meal walking is one of the most accessible tools for blood sugar balance. Even a short walk can help muscles take up glucose during the period when blood sugar is rising.
This does not need to be intense. A calm walk after lunch or dinner may be easier to sustain than a complicated training plan.

Prioritize sleep and circadian rhythm
Sleep loss can affect appetite regulation, insulin sensitivity, cravings, and energy expenditure. Late meals, irregular sleep timing, and short sleep may make it harder for the liver to manage incoming energy efficiently.
A realistic starting point is a consistent wake time, morning light exposure, and a calmer final hour before bed. These basics may support better metabolic regulation without adding another demanding rule.
Be thoughtful about dietary fat quality
Fat quality matters more than simply labeling fat as “good” or “bad.” Many people do better with a pattern built around olive oil, nuts, seeds, fish, legumes, and mostly whole foods.
For a practical nutrition next step, this guide on fat quality for liver health can help separate supportive food choices from common confusion.
Be honest about alcohol
Alcohol can contribute to liver stress and may interact with metabolic risk. Even when fatty liver is considered metabolic, alcohol intake can still matter.
Anyone with known liver fat should discuss alcohol patterns with a healthcare provider. The safest choice depends on liver status, fibrosis risk, medical history, and overall intake pattern.
What changes are realistic?
Progress with lean fatty liver is usually measured in patterns, not dramatic overnight changes. Many people first notice steadier energy, fewer post-meal crashes, better digestion, improved sleep, or stronger workouts.
Measurable changes may include improved triglycerides, fasting glucose, A1C, liver enzymes, waist measurement, or imaging findings. The timeline varies because liver fat, insulin sensitivity, muscle mass, alcohol exposure, medication use, and genetics all influence response.
| Timeframe | Possible early signal | What to avoid overinterpreting |
|---|---|---|
| 1–2 weeks | Fewer post-meal crashes, steadier hunger, better walk consistency | Daily weight fluctuations |
| 4–8 weeks | Better energy, improved training capacity, improved triglyceride pattern | One isolated lab result |
| 8–12+ weeks | More meaningful changes in average glucose markers or liver enzymes | Self-diagnosing liver fat without clinical follow-up |
Exercise training may support reductions in liver fat even when weight loss is modest or absent.[7] That is encouraging for lean adults who need better metabolic function, not a smaller body.
A practical 4-week plan for lean fatty liver support
This plan is educational and designed for generally healthy adults. Anyone with diabetes, liver disease, pregnancy, eating disorder history, significant medical conditions, or glucose-affecting medications should personalize changes with a qualified clinician.
Week 1: Create a baseline without judgment
- Track waist measurement once, not daily.
- Write down usual alcohol intake, sleep timing, and meal patterns.
- Add a 10-minute walk after one meal most days.
- Build one meal per day around protein, fiber, and a minimally processed carbohydrate.
This week is about awareness. Lean fatty liver is easier to address when patterns are visible rather than guessed.
Week 2: Upgrade carbohydrates instead of fearing them
- Swap sugary drinks for water, sparkling water, or unsweetened tea.
- Choose beans, oats, potatoes, fruit, lentils, or whole grains more often than refined snacks.
- Pair carbohydrates with protein, fiber, or healthy fats.
- Keep the post-meal walk habit in place.
The goal is a slower, steadier glucose response. This may support insulin sensitivity and reduce the liver’s pressure to handle repeated energy surges.
Week 3: Add strength training
- Complete two full-body strength sessions.
- Use bodyweight, machines, dumbbells, bands, or a coached program.
- Train with moderate effort and safe technique.
- Repeat the same exercises so progress is easy to notice.
Muscle is metabolic tissue. Building strength may help shift the focus away from weight and toward better glucose storage, function, and resilience.

Week 4: Tighten recovery and review signals
- Choose a consistent wake time for most days.
- Reduce late-night snacking if it is frequent.
- Review alcohol patterns honestly.
- Note energy, cravings, sleep, digestion, and workout performance.
At the end of four weeks, the question is not whether everything is solved. The question is which habits felt realistic enough to continue for another eight to twelve weeks.
Frequently Asked Questions
Can lean people really get lean fatty liver?
Yes. Lean fatty liver can occur in people with a normal BMI or slim appearance. It is often linked to visceral fat, insulin resistance, low muscle mass, genetics, alcohol exposure, or other metabolic factors. A normal weight does not automatically mean the liver is free from excess fat. A healthcare provider can help confirm the cause and assess fibrosis risk.
Is TOFI the same as fatty liver?
TOFI and fatty liver are related, but they are not exactly the same. TOFI describes a body composition pattern where someone appears thin but carries more internal or visceral fat. Fatty liver means excess fat has accumulated in liver cells. A TOFI pattern may increase risk, but imaging or medical evaluation is needed to identify fatty liver.
Can liver enzymes be normal with fatty liver?
Yes. Some people with fatty liver have ALT, AST, or GGT within the reference range. Liver enzymes can provide useful clues, but they do not always reflect liver fat amount or fibrosis risk. Clinicians may use imaging, non-invasive scores, and cardiometabolic risk assessment when fatty liver is suspected.
Should lean people with fatty liver try to lose weight?
Not always. For lean adults, aggressive weight loss may be unnecessary or inappropriate, especially if muscle mass is already low. The focus is often better placed on resistance training, protein adequacy, fiber-rich meals, lower alcohol exposure, improved sleep, and reduced visceral fat. A clinician or dietitian can tailor the goal to body composition, labs, and liver assessment.
What foods are most helpful for lean fatty liver support?
A helpful pattern usually emphasizes protein, vegetables, legumes, fruit, whole-food carbohydrates, nuts, olive oil, and fish when appropriate. Reducing sugary drinks, frequent refined snacks, and heavy alcohol intake may also support liver health. The best approach improves metabolic markers while still providing enough energy and protein. People with medical conditions should personalize nutrition changes with professional guidance.
Conclusion
A lean body can still carry hidden metabolic stress. Lean fatty liver is a reminder that liver health depends on fat distribution, insulin sensitivity, muscle, sleep, alcohol exposure, genetics, and daily movement patterns, not body weight alone.
The most useful next step is not panic or extreme restriction. It is a calmer strategy: confirm what is happening, build muscle, walk after meals, improve food quality, protect sleep, and review alcohol honestly.
When the focus shifts from “Do I look healthy?” to “Is my metabolism well supported?”, the path becomes more practical, measurable, and sustainable.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or treatment plan. TheMetabolicHub.com does not replace professional medical guidance.
References
- Kumar R, Mohan S. Non-alcoholic fatty liver disease in lean subjects: characteristics and implications. Journal of Clinical and Translational Hepatology. 2017. PMC: PMC5606968
- Tacke F, et al. EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease. Journal of Hepatology. 2024. PMID: 38851997
- Patel AH, et al. Nonalcoholic fatty liver disease in lean/nonobese and obese individuals: a comprehensive review on prevalence, pathogenesis, clinical outcomes, and treatment. Journal of Clinical and Translational Hepatology. 2023. PMID: 36643037
- Chen M, et al. Lean nonalcoholic fatty liver disease and sarcopenia. Frontiers in Endocrinology. 2023. PMID: 37424859
- Lin H, et al. Association of genetic variations with NAFLD in lean individuals. Journal of Clinical and Translational Hepatology. 2022. PMID: 34610207
- Rinella ME, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023. PMID: 36727674
- Stine JG, et al. Exercise Training Is Associated With Treatment Response in Liver Fat Content by Magnetic Resonance Imaging in Patients With Nonalcoholic Fatty Liver Disease. American Journal of Gastroenterology. 2023. PMID: 36705333