Difference Between Alcoholic and Non-Alcoholic Fatty Liver Disease
Persistent fatigue, a sluggish feeling after meals, or unexplained discomfort under the right rib — these are the kinds of symptoms that are easy to dismiss as stress or aging. But for millions of people, they may signal something happening inside the liver long before any diagnosis is made. Two of the most common liver conditions today share a name — fatty liver disease — yet they have very different causes, timelines, and paths forward. Understanding what sets them apart may be the first step toward protecting your long-term health.
What Is the Difference Between Alcoholic and Non-Alcoholic Fatty Liver Disease?
Alcoholic fatty liver disease (ALD) is caused primarily by regular, heavy alcohol consumption that overloads the liver’s ability to process fat and repair itself. Non-alcoholic fatty liver disease (NAFLD) — now increasingly called metabolic-associated fatty liver disease (MAFLD) — is driven by metabolic factors such as insulin resistance, obesity, and type 2 diabetes, and is currently the leading cause of chronic liver disease worldwide, affecting approximately 1 in 3 adults. Both conditions follow a similar progression from fat accumulation to inflammation, fibrosis, and potentially cirrhosis — but ALD tends to progress faster, typically over 10 years versus roughly 30 years for NAFLD.
| Feature | ALD (Alcoholic) | NAFLD (Non-Alcoholic) |
|---|---|---|
| Primary cause | Regular heavy alcohol use | Insulin resistance, obesity, metabolic syndrome |
| Global prevalence | Tied to alcohol consumption rates | ~1 in 3 adults worldwide |
| Typical progression to cirrhosis | ~10 years | ~30 years |
| Lifetime cirrhosis risk | ~22% | ~1.2% |
| Primary intervention | Abstinence + nutrition support | Weight loss + metabolic management |
| Early stages reversible? | Yes, with abstinence | Yes, with lifestyle changes |
Key Takeaways
- Both ALD and NAFLD begin with excess fat accumulation in the liver but have distinct root causes and treatment paths.
- NAFLD now affects roughly 1 in 3 adults globally — making it the most common liver condition.
- ALD progresses more rapidly: cirrhosis may develop in ~10 years versus ~30 years for NAFLD.
- Early-stage damage in both conditions is often reversible with the right lifestyle interventions.
- Once significant scarring (fibrosis or cirrhosis) develops, changes are largely permanent — making early detection critical.
How the Liver Gets Overwhelmed
The liver is one of the body’s most hardworking organs — managing over 500 distinct functions including filtering toxins from the blood, converting nutrients into usable energy, producing bile for digestion, and supporting immune function. When the liver can no longer process excess fat efficiently, fat begins to accumulate in liver cells. This is the starting point for both ALD and NAFLD.
Both conditions follow the same four-stage progression: fat buildup (steatosis) → inflammation (steatohepatitis) → scarring (fibrosis) → cirrhosis. The critical difference lies in what triggers this chain — and how quickly it advances.
Alcoholic Fatty Liver Disease: What Drives It
For people with ALD, the liver’s burden comes directly from ethanol. Each time alcohol is metabolized, it generates toxic byproducts that damage liver cells, trigger inflammation, and gradually replace healthy tissue with scar tissue. This cycle repeats with every drink.
The CDC defines heavy drinking as more than 14 standard drinks per week for men and more than 7 per week for women — where one standard drink equals 12 oz of beer, 5 oz of wine, or 1.5 oz of spirits. Daily heavy consumption typically poses a higher cumulative risk than occasional binge drinking.[1]
The encouraging reality: for many people, early ALD is reversible. Complete abstinence — combined with adequate nutrition and medical support — significantly improves outcomes, even in cases with some degree of scarring.
Non-Alcoholic Fatty Liver Disease: The Metabolic Connection
NAFLD develops without alcohol as a cause. Instead, it is closely tied to the cluster of metabolic conditions — insulin resistance, obesity, elevated triglycerides, and type 2 diabetes — that define metabolic syndrome. When cells become resistant to insulin, the body compensates by releasing more insulin, which signals the liver to store more fat.[2]
The numbers are striking: research suggests that 75–92% of people with obesity and 60–70% of those with obesity-related type 2 diabetes have NAFLD. This condition is not exclusive to adults — studies have found early changes in nearly 10% of children, underscoring the role of metabolic health at every life stage.
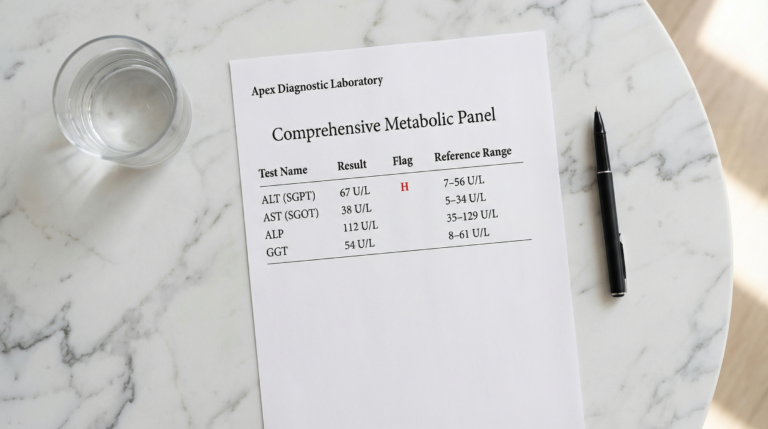
This cycle can develop quietly over years — which is why so many people are caught off guard when a doctor mentions elevated liver enzymes. It is not a personal failure. It is a metabolic pattern that can be addressed once it is understood.
Comparing Progression and Risk
One of the most clinically important distinctions between ALD and NAFLD is the speed of progression. Research indicates that alcohol-related liver damage typically reaches cirrhosis in approximately 10 years of ongoing heavy use — compared to roughly 30 years for the metabolic-driven form.[3]
Lifetime cirrhosis risk also differs significantly: approximately 22% for ALD versus around 1.2% for NAFLD. The risk of hepatocellular carcinoma (liver cancer) follows a similar pattern — about 7% at 5–10 years for ALD, versus 0–3% over 20 years for NAFLD.
Importantly, both conditions can remain stable for years — or progress rapidly depending on individual risk factors including genetics, diet, physical activity, and whether underlying metabolic conditions are managed.
Recognizing the Signs Early
Early-stage fatty liver disease often produces no clear symptoms — which is what makes it so easy to miss. When early signs do appear, they tend to be nonspecific: persistent fatigue, mild discomfort below the right rib cage, or reduced appetite. Many people attribute these to stress or a busy schedule.
As the condition advances, more distinct signs emerge — yellowing of the skin or eyes (jaundice), swelling in the abdomen or legs from fluid accumulation, easy bruising, and cognitive changes if the liver can no longer effectively clear toxins. Spider-like veins on the skin and hormonal changes in men are more specific to ALD.
If any of these symptoms are present — especially in someone with metabolic syndrome, obesity, or a pattern of heavy alcohol use — blood tests and imaging should be discussed with a clinician promptly.
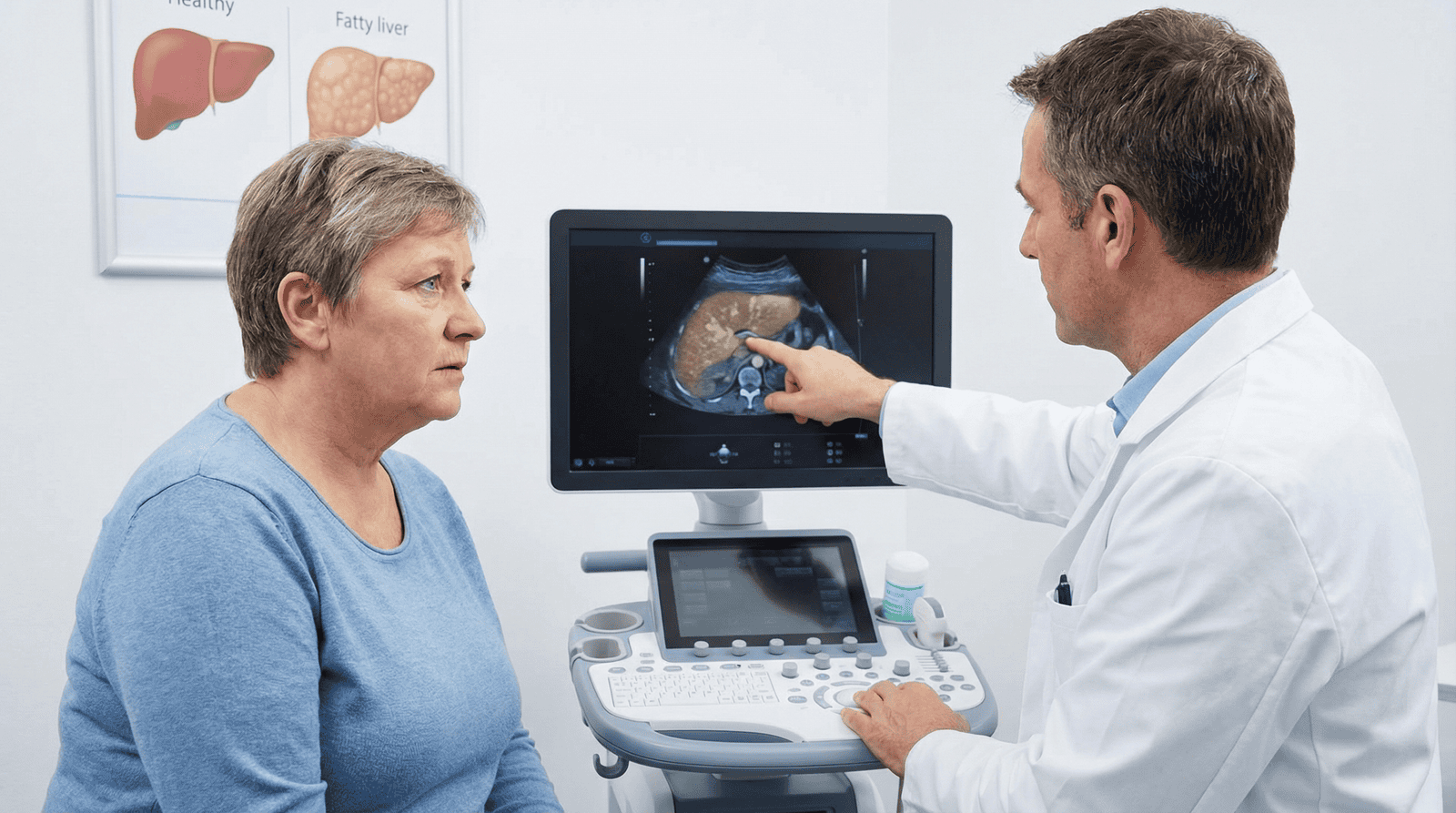
Diagnosis: What to Expect
Diagnosis typically begins with a medical history — including alcohol use patterns, metabolic risk factors, and family history — followed by targeted blood tests and imaging. Ultrasound is the most commonly used first-line imaging tool; Fibroscan (a noninvasive stiffness test) can estimate the degree of fibrosis without a needle.[4]
Liver biopsy remains the gold standard for confirming diagnosis and staging fibrosis, but it is invasive and typically reserved for cases where noninvasive testing is inconclusive or treatment decisions depend on precise staging. One study found that clinical findings matched biopsy results with approximately 91% sensitivity in people with elevated liver enzymes — supporting the use of noninvasive tools as the first step.
Lifestyle Changes That Make a Difference
The most powerful interventions for both ALD and NAFLD center on lifestyle — and the evidence is compelling. For NAFLD, research suggests that losing just 3–5% of body weight may reduce liver fat accumulation, while 5–7% weight loss may help resolve steatohepatitis (liver inflammation) in many people.[5]
Practically speaking, that translates to: prioritizing whole foods — leafy greens, broccoli, peppers, zucchini, berries, legumes — alongside quality proteins like eggs, fish, and Greek yogurt. Minimizing ultra-processed foods, refined carbohydrates, and added sugars reduces the metabolic load on the liver.
For movement, research supports 150 minutes of moderate activity per week — roughly 20–25 minutes daily. Even short walks after meals may help reduce post-meal blood sugar spikes, which directly affects liver fat metabolism. A combination of aerobic activity and light resistance training appears most effective.
For ALD, the primary intervention is complete abstinence from alcohol. When paired with nutritional support and medical monitoring, abstinence has been shown to improve liver function meaningfully — even in people with some degree of scarring.
Medical Treatment Options
For ALD with active inflammation, corticosteroids may be prescribed to reduce inflammation — though research suggests approximately 40% of patients do not respond. Pentoxifylline is used as a second-line option when steroids are not appropriate.
For NAFLD with concurrent type 2 diabetes, certain metabolic agents — including thiazolidinediones and GLP-1 receptor agonists such as liraglutide — may support both blood sugar control and liver fat reduction. Emerging therapies targeting cell death pathways (including emricasan, a pancaspase inhibitor) and fibrosis-driving immune signals (ASK1 inhibitors, CCR2/CCR5 blockers) are currently in clinical trials and show early promise.[6]
No pharmacological approach replaces lifestyle intervention — but for people with advanced metabolic risk, combining both may offer the best outcomes.
Can These Conditions Be Reversed?
Early-stage fatty liver disease — particularly simple steatosis — is often reversible with sustained lifestyle changes. For ALD, abstinence is the cornerstone of recovery. For NAFLD, losing 5–10% of body weight through a balanced diet and regular movement typically leads to measurable improvement in both liver fat and inflammation markers.
The critical caveat: once significant fibrosis or cirrhosis has developed, the structural changes to the liver are largely permanent. At that stage, the focus shifts to slowing further progression, managing complications, and — in advanced cases — evaluating eligibility for transplant. This is precisely why early detection and early action matter so much.
Conclusion
Alcoholic and non-alcoholic fatty liver disease share a common endpoint but follow very different paths to get there. ALD is driven by alcohol consumption and tends to progress faster; NAFLD is rooted in metabolic dysfunction and is now the most common liver condition in the world. Both are serious — and in their early stages, both are addressable.
Many people who felt stuck with vague symptoms and confusing test results have found that understanding what is actually happening in their liver was the turning point. Early lifestyle changes — real food, consistent movement, reducing alcohol, addressing metabolic risk factors — remain the most powerful tools available.
Frequently Asked Questions
What is the main difference between alcoholic and non-alcoholic fatty liver disease?
The primary difference is the underlying cause. Alcoholic fatty liver disease (ALD) is driven by regular, heavy alcohol consumption that overwhelms the liver’s processing capacity. Non-alcoholic fatty liver disease (NAFLD) develops without significant alcohol use and is instead linked to metabolic factors — particularly insulin resistance, obesity, and type 2 diabetes. Both cause fat to accumulate in liver cells and can progress through similar stages, but ALD typically advances more rapidly and carries a higher lifetime risk of cirrhosis (~22% vs ~1.2% for NAFLD).
Can fatty liver disease be reversed?
In its early stages — particularly simple fat accumulation (steatosis) without significant inflammation or scarring — fatty liver disease may be reversible. For ALD, research suggests that complete abstinence from alcohol, combined with nutritional support, can significantly improve liver function. For NAFLD, losing 5–10% of body weight through diet and exercise may support meaningful reduction in liver fat and inflammation. Once significant scarring (fibrosis or cirrhosis) has developed, the structural changes are largely permanent, though progression can often be slowed.
What are the early warning signs of fatty liver disease?
Early-stage fatty liver disease often produces no clear symptoms — which is why it frequently goes undetected without routine blood tests. When symptoms do appear, they tend to be nonspecific: persistent fatigue, mild discomfort or a dull ache below the right rib cage, low appetite, or mild nausea. Elevated liver enzymes on a standard blood panel (ALT, AST) are often the first measurable signal. Anyone with risk factors — including metabolic syndrome, obesity, type 2 diabetes, or heavy alcohol use — should discuss proactive screening with their healthcare provider.
How is non-alcoholic fatty liver disease connected to insulin resistance?
Insulin resistance is one of the core drivers of NAFLD. When cells stop responding efficiently to insulin, the body compensates by producing more of it — and elevated insulin signals the liver to store more fat. Over time, this leads to fat accumulation in liver cells, which can trigger inflammation and eventually scarring. Research suggests that 75–92% of people with obesity and 60–70% of those with obesity-related type 2 diabetes have NAFLD, highlighting the deep connection between metabolic dysfunction and liver health.
What lifestyle changes are most effective for fatty liver disease?
Evidence consistently points to diet and movement as the most impactful levers. For NAFLD, research suggests that losing 3–5% of body weight may reduce liver fat, while 5–7% may help resolve active liver inflammation. Prioritizing whole foods — vegetables, legumes, lean proteins like fish and eggs — while reducing ultra-processed foods and refined carbohydrates directly supports liver metabolic function. Roughly 150 minutes of moderate movement per week (about 20–25 minutes daily) appears beneficial. For ALD, complete abstinence from alcohol is the single most important step and can lead to meaningful recovery even in moderate-stage disease.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or treatment plan. TheMetabolicHub.com does not replace professional medical guidance.
References
- Rehm J et al. Alcohol use and the risk of liver cirrhosis: a systematic review and meta-analysis. American Journal of Gastroenterology. 2010. PMID: 20179695
- Neuschwander-Tetri BA. Hepatic lipotoxicity and the pathogenesis of nonalcoholic steatohepatitis: The central role of nontriglyceride fatty acid metabolites. Hepatology. 2010. PMID: 20648554
- Teli MR et al. Determinants of progression to cirrhosis or fibrosis in pure alcoholic fatty liver. Lancet. 1995. PMID: 7658347
- Castera L et al. Noninvasive assessment of liver fibrosis in chronic hepatitis C. Hepatology. 2005. PMID: 15723574
- Vilar-Gomez E et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology. 2015. PMID: 25865049
- Ratziu V et al. Elafibranor, an agonist of the peroxisome proliferator-activated receptor-α and -δ, induces resolution of nonalcoholic steatohepatitis without fibrosis worsening. Gastroenterology. 2016. PMID: 26874076