What Your Liver Enzyme Results Actually Mean — ALT, AST, ALP & GGT Explained
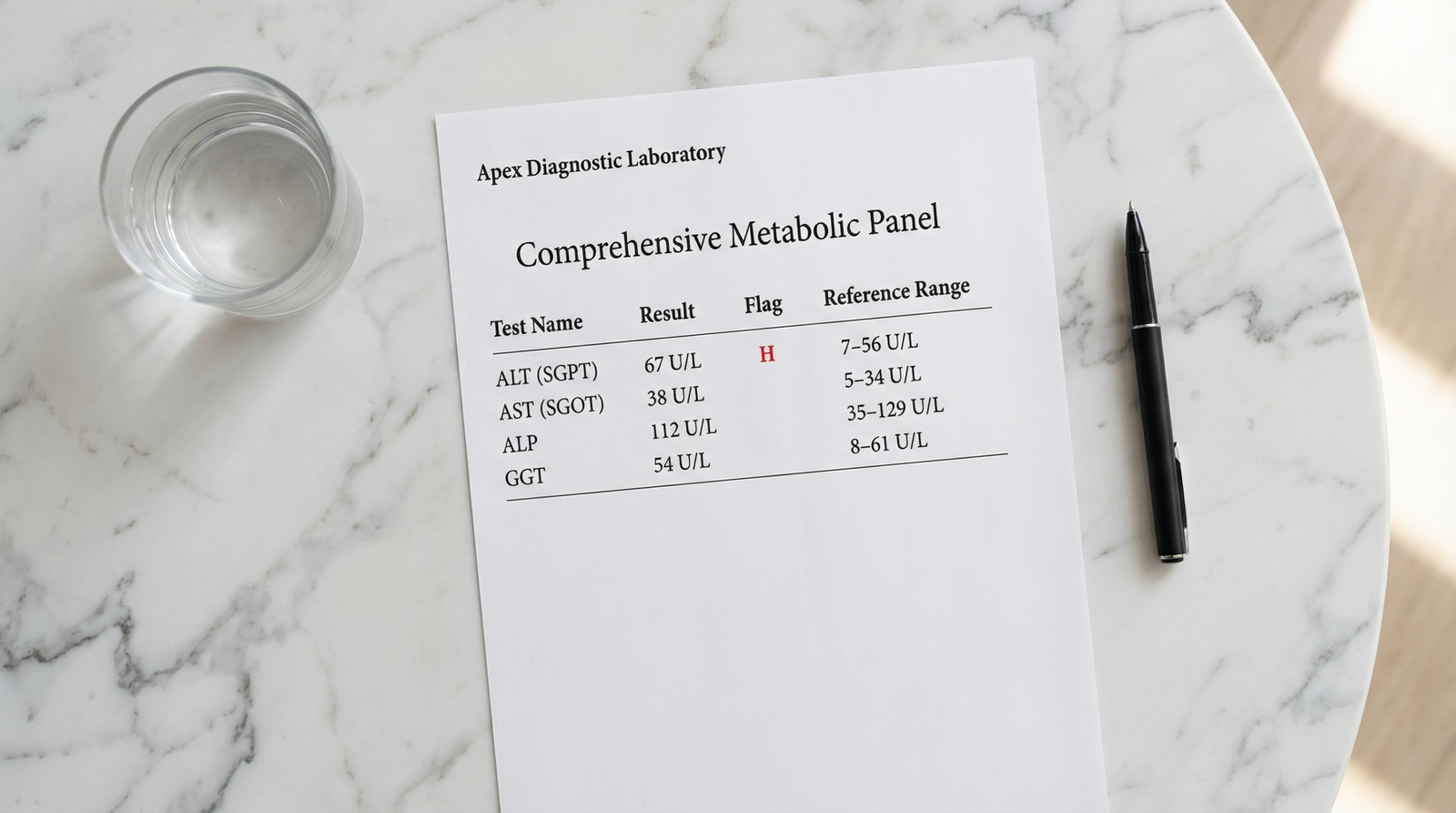
You get your blood work back. The liver section has some flagged numbers. Now you’re sitting with a printout full of abbreviations and reference ranges, trying to figure out if this is something to worry about — or not.
Here’s what your liver enzymes actually mean — explained clearly, the way it should have been done in the office.
Liver enzymes are among the most commonly ordered tests in routine bloodwork — and among the most commonly misunderstood. Most people either dismiss a mildly elevated result (“the doctor didn’t seem worried”) or spiral into worst-case scenarios. The reality is almost always somewhere in between, and considerably more nuanced than a flagged number on a printout suggests.
What these tests actually measure is how much of certain proteins have leaked out of your liver cells into your bloodstream. Healthy liver cells contain these enzymes. When cells are damaged or stressed, the enzymes escape. The question is always: how much, which ones, and why?
What You’ll Know After Reading This
- What ALT, AST, ALP, and GGT each measure — and why they’re different
- What “normal range” actually means, and why it varies between labs
- The most common reasons these numbers rise — many of them benign
- When a mildly elevated result needs attention vs. when it can be monitored
- What the AST:ALT ratio can tell you that individual numbers can’t
- Specific questions to ask your doctor at your next appointment
Liver Enzymes Explained: What ALT, AST, ALP and GGT Each Measure
These four enzymes appear on most standard liver function panels. They’re not interchangeable — each one tells a slightly different story about what’s happening in your liver (and sometimes, beyond it).[1]
| Enzyme | Full Name | Primary Location | Normal Range (Women) | Normal Range (Men) | What Elevation Suggests |
|---|---|---|---|---|---|
| ALT | Alanine Aminotransferase | Liver (most specific) | 7–35 U/L | 7–56 U/L | Liver cell damage or inflammation |
| AST | Aspartate Aminotransferase | Liver, heart, muscles | 10–35 U/L | 10–40 U/L | Liver or muscle injury; ratio to ALT is key |
| ALP | Alkaline Phosphatase | Liver bile ducts, bone | 44–147 U/L | 44–147 U/L | Bile duct obstruction or bone-related cause |
| GGT | Gamma-Glutamyl Transferase | Liver, bile ducts, kidneys | 8–61 U/L | 8–61 U/L | Alcohol use, bile duct issue, or medication effect |
Normal ranges vary between labs — always compare your result against the reference range printed on your own lab report, not a generic number found online. That said, the sex-based difference in ALT and AST thresholds is clinically meaningful: men naturally have somewhat higher muscle mass, which affects baseline enzyme levels. A value that sits comfortably within the male reference range might be worth closer attention in a woman.[1]
ALT — The Most Liver-Specific Marker
ALT is found predominantly in liver cells, which makes an elevated reading a fairly direct signal that something is affecting the liver specifically. It’s the first number clinicians look at when liver health is the question.
It rises with fatty liver disease, viral hepatitis, alcohol use, certain medications — including common over-the-counter drugs like acetaminophen — and acute liver injury. It can also spike temporarily after intense exercise, which is a normal physiological response, not a sign of damage.[1]
One nuance worth knowing: some researchers now argue that the traditional ALT cutoffs were calibrated on populations that included people with undiagnosed fatty liver disease — meaning the “normal” threshold may be set higher than optimal for detecting early metabolic liver stress. This applies to both sexes, though it’s particularly relevant for women, whose reference range is already lower than men’s.
AST — Context-Dependent
AST is also found in heart muscle, skeletal muscle, kidneys, and brain tissue. That’s why an isolated AST elevation — without a corresponding ALT rise — often points away from the liver entirely. It might reflect muscle damage from a hard workout, a cardiac event, or a thyroid condition.[2]
Neither enzyme tells the full story on its own. The pattern — and the ratio between them — matters as much as the individual number.
ALP — The Bile Duct Signal
Rather than flagging liver cell injury, elevated ALP more often signals a problem in the bile ducts — the channels that carry bile from the liver to the small intestine. When those ducts become blocked or inflamed, ALP rises.
ALP is also produced by bone, which is clinically important: elevated ALP without a corresponding rise in GGT often points to a bone-related cause rather than a liver issue. In women, ALP can be temporarily elevated during pregnancy due to placental production — a normal variation, not liver disease.[3]
GGT — The Sensitive Early Warning
GGT is typically the first liver enzyme to rise when bile ducts are under pressure — often before symptoms appear and before other markers shift. That early-warning quality makes it useful, but its lack of specificity limits what it can tell you alone.
Where GGT earns its place: when ALP is elevated, an accompanying GGT rise confirms the issue is liver- or bile duct-related, not bone-related. That single distinction guides what happens next.[3]
How to Read the Numbers: What “Elevated” Actually Means
A result flagged as “high” simply means it’s above the lab’s reference range. What matters more is how far above normal, and which pattern of elevations you’re seeing. A number 10% above the upper limit of normal is a very different situation from a number three times the upper limit.
| Level of Elevation | Classification | Common Causes | Recommended Action |
|---|---|---|---|
| Within range | Normal | No liver cell leakage detected | No action needed |
| 1–3× upper limit | Mildly elevated | Fatty liver, alcohol, medication, intense exercise, recent illness | Repeat test in 4–8 weeks; lifestyle review |
| 3–10× upper limit | Moderately elevated | MASLD, hepatitis, medication toxicity, significant alcohol use | Follow-up imaging (ultrasound); investigate cause |
| >10× upper limit | Significantly elevated | Acute hepatitis, drug-induced liver injury, ischemic hepatitis | Prompt medical evaluation — do not wait |
Reference ranges are set to capture 95% of healthy people — which means 5% of completely healthy individuals will fall outside the “normal” range by chance alone. A single mildly elevated result, especially in isolation, is often not significant. This is particularly true if you exercised hard recently, had a viral illness, or started a new supplement.[1]
The Most Common Reasons Liver Enzymes Rise
For women in the 35–55 age range, the most frequently overlooked cause is metabolic dysfunction-associated steatotic liver disease (MASLD — formerly called NAFLD), now estimated to affect roughly 1 in 3 adults in the US.
It develops silently, often without symptoms, and is directly linked to insulin resistance and blood sugar dysregulation. This is not a personal failure — MASLD typically develops over years, driven by dietary patterns, sleep disruption, and metabolic stress rather than any single choice.[4]
Medication and supplement use is the other frequently missed category. Many common drugs — including statins, NSAIDs like ibuprofen, and even high-dose vitamins — can raise liver enzymes without causing meaningful liver damage. The same applies to certain herbal products often assumed to be safe simply because they’re “natural.”
| Category | Common Causes | Typically Reversible? |
|---|---|---|
| Very common | Fatty liver (MASLD), alcohol, obesity, intense exercise, NSAIDs, statins, high-dose vitamins, thyroid dysfunction | Yes — with lifestyle or medication changes |
| Less common | Viral hepatitis (A, B, C), autoimmune hepatitis, celiac disease, gallstones, Wilson’s disease, hemochromatosis | Depends on underlying condition |
| Supplement-related | Green tea extract, kava, comfrey, high-dose niacin, vitamin A, certain weight-loss products | Usually yes, once stopped |
The AST:ALT Ratio — A Number Most People Never Check
Individual enzyme values tell you that something may be off. The ratio between AST and ALT often tells you what. Research consistently supports this ratio as a useful diagnostic pointer — worth knowing whether or not your doctor mentions it.[2]
| AST:ALT Ratio | What It Suggests | Clinical Significance |
|---|---|---|
| < 1.0 | ALT higher than AST | Classic pattern for MASLD or viral hepatitis. Often reversible with lifestyle changes. |
| 1.0–2.0 | Borderline | Could reflect progressing MASLD or early alcohol-related changes. Clinical history is essential. |
| > 2.0 | AST more than twice ALT | Strongly associated with alcohol-related liver disease — present in ~90% of alcoholic hepatitis cases.[2] |
A single elevated number on a lab panel is not a diagnosis. It’s a signal — one piece of information that points in a direction and asks a question. The answer always requires more context.
Lifestyle Factors That Move These Numbers
Several everyday factors shift liver enzyme levels — and knowing them helps you interpret your results more accurately.
Alcohol is the most predictable: regular consumption raises GGT and tends to elevate AST disproportionately to ALT. Even moderate intake within what many consider acceptable can cause persistent mild elevation.
Exercise is a less obvious factor. Intense resistance training can significantly raise both AST and ALT in the 24–72 hours following a workout, because these enzymes are also present in muscle tissue. A blood draw taken shortly after a hard session may show elevations that have nothing to do with the liver.
Diet plays a direct role. Excess sugar — particularly fructose from sugar-sweetened beverages — is processed in the liver via a pathway that increases fat production and triglycerides.[5] Over time, this contributes to fat accumulation in liver cells and rising ALT. Removing sugar-sweetened beverages is one of the most direct dietary changes for improving liver enzyme levels.
Sleep matters more than most people expect. Chronic sleep restriction raises cortisol and disrupts the hormonal environment that regulates blood sugar and fat metabolism — both of which affect liver enzyme levels over time. Research from the Journal of Applied Physiology showed that even one week of restricted sleep produced significant alterations in glucose tolerance and insulin sensitivity.[6] If your sleep has been consistently poor, that’s a relevant factor to mention alongside your lab results.
When to Follow Up — and How Urgently
Seek prompt medical attention if elevated enzymes are accompanied by yellowing of the skin or eyes (jaundice), severe abdominal pain (especially upper right), dark urine or very pale stools, significant nausea or vomiting lasting more than a few days, sudden extreme fatigue, or values more than 10× the upper limit of normal.
For mildly elevated results without symptoms, the standard approach is to repeat the test in 4–8 weeks after addressing the most obvious potential contributors: reducing alcohol, stopping non-essential supplements, avoiding NSAIDs where possible, and reducing sugar intake. If the elevation persists, further investigation — typically an abdominal ultrasound and an expanded blood panel — is the appropriate next step.
If Your Results Came Back Elevated — Here’s What to Do Next
Don’t panic over a single mildly elevated result. One data point without symptoms or context is rarely meaningful on its own. Start by reviewing the obvious causes: recent intense exercise, alcohol in the 48–72 hours before the test, new supplements or medications, or a recent illness.
Give it 4–8 weeks of addressing those potential causes, then retest. This alone resolves many mildly elevated results. If it persists, ask your doctor about an abdominal ultrasound — it’s the standard next step and provides much more information about what’s actually happening. Also ask for a full liver panel if you only had ALT and AST — adding ALP, GGT, bilirubin, and albumin gives a considerably more complete picture.
Questions worth asking your doctor: “How far above normal are these values — are we talking 10% or three times the limit?” And: “At what point would you want to investigate further, and what would that look like?”
Conclusion
Liver enzyme results are not a verdict. They’re a data point — your body signaling that something is worth paying attention to, not necessarily that something is seriously wrong.
Understanding what ALT, AST, ALP, and GGT each measure — and what their patterns mean together — puts you in a much better position to have an informed conversation with your doctor. The liver is remarkably resilient. Caught early, most enzyme elevations respond well to targeted lifestyle changes. That’s worth knowing.
Frequently Asked Questions
What do elevated liver enzymes actually mean?
Elevated liver enzymes mean that more of these proteins than usual have leaked from liver cells into your bloodstream — a sign that something is stressing or damaging those cells. The cause can be minor and temporary (intense exercise, a recent illness, a new medication) or more significant (fatty liver disease, viral hepatitis). A single mildly elevated result in isolation is often not meaningful. The pattern across all four enzymes, the degree of elevation, and whether it persists over time are what matter most.
Can liver enzymes go back to normal on their own?
Yes, in many cases. Mildly elevated enzymes caused by fatty liver disease, alcohol, or medication use often normalize within weeks to months when the underlying cause is addressed. Research on metabolic fatty liver disease specifically shows meaningful improvement in liver enzyme levels with dietary changes and regular movement — even without dramatic weight loss. This is one reason doctors often recommend retesting before pursuing further investigation.
What is the difference between ALT and AST?
ALT is found predominantly in the liver, making it the more liver-specific marker — an elevated ALT almost always points directly at the liver. AST is also found in heart muscle, skeletal muscle, and other tissues, so an isolated AST elevation doesn’t automatically mean a liver problem. The ratio between them carries diagnostic weight: when AST is more than twice as high as ALT, alcohol-related liver disease becomes a more likely explanation. When ALT is higher, fatty liver disease or viral hepatitis are more common causes.
Do supplements affect liver enzyme levels?
Yes — more commonly than most people realize. High-dose vitamin A, niacin (vitamin B3), and iron supplements can all raise liver enzymes. Certain herbal supplements — including green tea extract, kava, comfrey, and some weight-loss products — are well-documented causes of drug-induced liver injury. If you take supplements regularly and have elevated liver enzymes, mention this to your doctor. Stopping non-essential supplements for 4–6 weeks before retesting can help clarify whether they’re contributing.
Should I be worried about slightly elevated GGT?
Mildly elevated GGT alone is rarely cause for alarm. GGT is highly sensitive and rises with alcohol, many medications, obesity, smoking, and even regular caffeine intake. Its main clinical value is as a cross-check alongside ALP — elevated ALP combined with elevated GGT confirms the liver, not bone, as the source of the elevation. Chronically elevated GGT, even mildly, has been associated with cardiovascular risk in population studies, so it’s worth monitoring over time rather than dismissing entirely.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or treatment plan. TheMetabolicHub.com does not replace professional medical guidance.
References
- Patel NJ, et al. Abnormal liver enzymes: A review for clinicians. World J Gastroenterol. 2021. PMID: 34866905
- Giannini EG, et al. Liver enzyme alteration: a guide for clinicians. CMAJ. 2005. PMID: 15684121
- Lala V, et al. Liver Function Tests. StatPearls. 2023. PMID: 29494096
- Chalasani N, et al. The diagnosis and management of nonalcoholic fatty liver disease. Hepatology. 2018. PMID: 28714183
- Malik VS, et al. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes. Diabetes Care. 2010. PMID: 20693348
- Spiegel K, et al. Sleep loss: a novel risk factor for insulin resistance and type 2 diabetes. J Appl Physiol. 2005. PMID: 16227462