Metabolic Syndrome Blood Tests: Which Labs to Track and Why
You get your labs back, and the numbers look… fine? Normal, mostly. But something still feels off — fatigue that doesn’t lift, a waistline that keeps creeping up, energy that crashes after lunch.
What your standard checkup may not have flagged is a cluster of metabolic signals that often show up quietly, one marker at a time. These patterns — elevated triglycerides, creeping blood sugar, low HDL — can reflect early metabolic dysfunction long before any single number crosses into “abnormal” territory.
That’s exactly why knowing which metabolic syndrome blood tests to track, and what each one actually means, matters more than most people realize. The encouraging news: these are some of the most actionable labs available. Understanding them turns a confusing printout into a clear roadmap.
Quick Win: Before your next blood draw, ask your doctor for a fasting panel — fasting glucose, fasting insulin, a full lipid panel, and hs-CRP. These four together give a far more complete metabolic picture than a standard lipid check alone.
What Metabolic Syndrome Blood Tests Actually Measure
Metabolic syndrome isn’t a single disease — it’s a cluster of five interconnected risk factors that, when three or more appear together, significantly raise the risk of type 2 diabetes and cardiovascular disease.
The National Cholesterol Education Program (NCEP ATP III) criteria — still the most widely used in clinical practice in the US — identify metabolic syndrome when any three of these five markers are present:[1]
| Marker | Threshold (NCEP ATP III) |
|---|---|
| Waist circumference | ≥40 in. (men) / ≥35 in. (women) |
| Triglycerides | ≥150 mg/dL |
| HDL cholesterol | <40 mg/dL (men) / <50 mg/dL (women) |
| Blood pressure | ≥130/85 mm Hg |
| Fasting blood glucose | ≥100 mg/dL |
Three of five is the threshold. That’s the part most people don’t hear until something bigger has already developed — which is why tracking these markers proactively, rather than waiting for a symptom, makes such a difference.[2]
The full diagnostic criteria for metabolic syndrome go deeper into how these markers interact and what your doctor is actually watching for.
The Core Metabolic Syndrome Blood Tests — Panel by Panel
A standard metabolic workup for syndrome risk typically covers three areas: lipids, glucose metabolism, and blood pressure. Here’s what each panel is actually measuring and why it matters.
Lipid Panel: Triglycerides and HDL Cholesterol
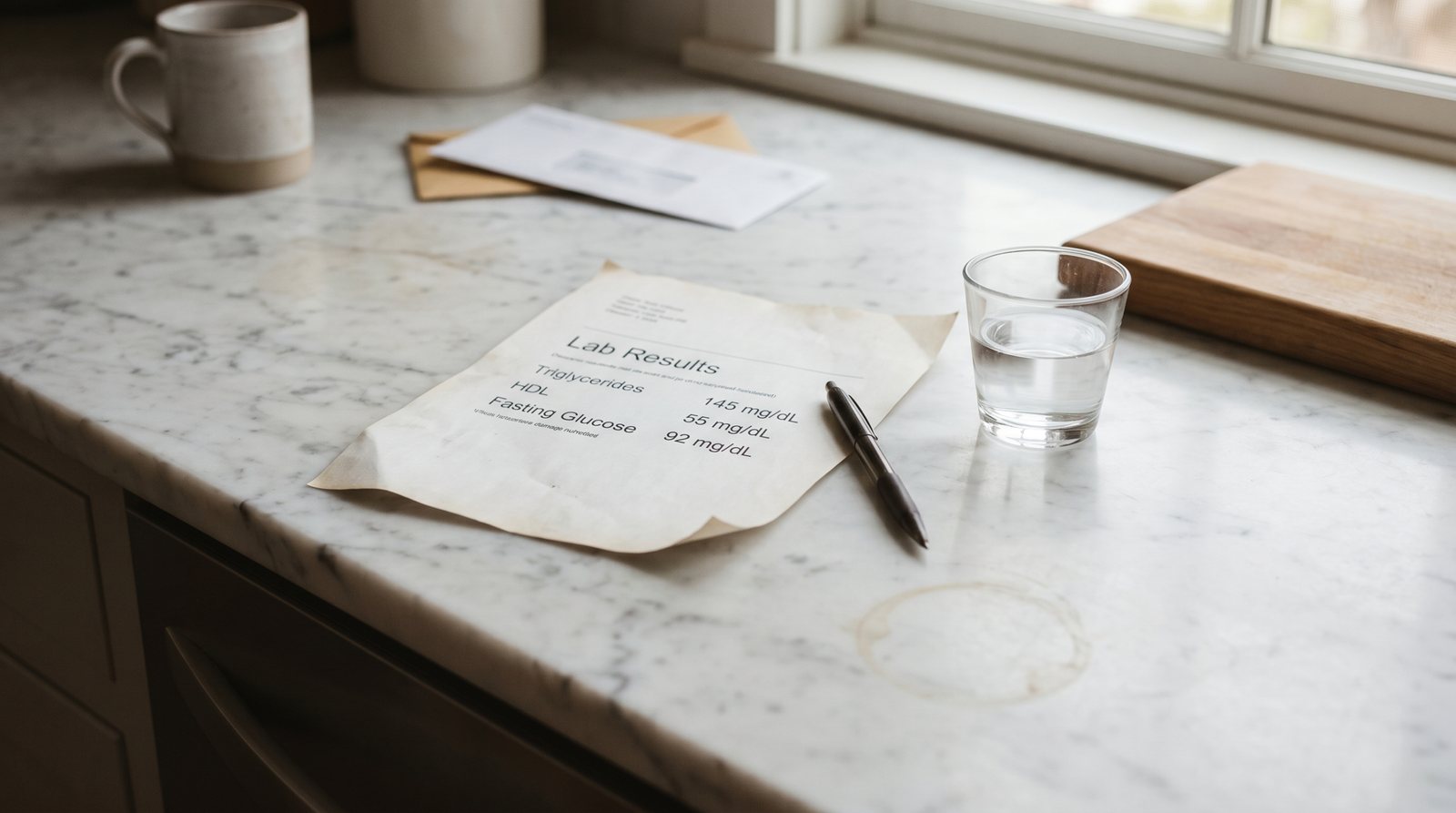
A full lipid panel checks total cholesterol, LDL, HDL, and triglycerides. For metabolic syndrome specifically, the two numbers that matter most are triglycerides and HDL.
Triglycerides above 150 mg/dL suggest the liver is processing excess carbohydrates or fats in a way that strains the metabolic system. HDL below 50 mg/dL (women) or 40 mg/dL (men) signals reduced capacity to clear fats from the bloodstream.
One pattern worth knowing: the ratio of triglycerides to HDL cholesterol is a useful proxy for insulin resistance. A TG:HDL ratio above 3.0 has been associated with insulin resistance even when fasting glucose looks normal — which makes it one of the more informative calculations available from a standard panel.[3]
Fasting Glucose and Insulin: The Blood Sugar Picture
Fasting glucose is the most common blood sugar check. A result between 100–125 mg/dL is classified as impaired fasting glucose — the prediabetes range. At 126 mg/dL or above on two separate draws, the threshold for a type 2 diabetes diagnosis is met.
What standard panels often miss: fasting insulin. This number isn’t automatically included in most routine labs, but it’s worth requesting. When fasting glucose sits in the high-normal range (95–100 mg/dL) but fasting insulin is elevated, that combination suggests the pancreas is already compensating — a sign of early insulin resistance before glucose crosses any diagnostic line.
HbA1c: The Three-Month Average
HbA1c reflects average blood glucose over approximately three months. Below 5.7% is considered normal; 5.7–6.4% falls in the prediabetes range; 6.5% or higher meets the American Diabetes Association’s threshold for a diabetes diagnosis.[4]
For people managing metabolic syndrome risk, HbA1c adds useful context that a single fasting glucose reading can’t provide. A fasting glucose of 98 mg/dL with an HbA1c of 5.9% tells a different story than the same fasting glucose with an HbA1c of 5.4%.
Blood Pressure: The Marker That Doesn’t Require a Lab
Blood pressure doesn’t show up on a blood draw, but it’s one of the five official diagnostic criteria. The threshold for metabolic syndrome is ≥130/85 mm Hg — or currently taking antihypertensive medication.
If blood pressure is a concern, tracking it over several mornings at rest gives a more accurate picture than a single clinical measurement. Two readings taken at the same office visit can look different from what a home monitor captures over two weeks.
How to Read Your Results — Without Overreacting to Single Numbers
Here’s something the standard health article tends to skip over: a single out-of-range value doesn’t mean much on its own. Metabolic syndrome is defined by a pattern, not a single number crossing a threshold.
One thing worth pushing back on here: the conventional framing of lab results as pass/fail. A triglyceride of 152 mg/dL isn’t meaningfully different from 148 mg/dL — but a triglyceride that has moved from 110 to 150 over 18 months, alongside HDL that’s dropped from 55 to 47, is a signal worth acting on even if nothing has technically crossed a cutoff yet.
Trend matters more than a single snapshot. What changed since the last draw? What direction are things moving? That context is often more useful than whether a number is technically “in range” today.
Reference Ranges vs. Optimal Ranges
Lab reference ranges are set based on population averages, not on what’s optimal for metabolic health. A fasting glucose of 95 mg/dL is “normal” by reference range standards — but research consistently shows that risk for insulin resistance increases incrementally starting around 90 mg/dL.
An HDL of 51 mg/dL technically clears the threshold for women — but HDL closer to 60 mg/dL or above is more strongly associated with cardiovascular protection. The goal isn’t just to pass the threshold. It’s to understand where on the spectrum each marker sits, and whether the overall pattern is moving in a positive direction.
Understanding Triglycerides, HDL, and Blood Pressure Together
These three markers interact in ways a single reading doesn’t capture. High triglycerides combined with low HDL — sometimes called “atherogenic dyslipidemia” — is a more concerning pattern than either value in isolation.
The American Heart Association identifies this combination as particularly relevant for cardiovascular risk, especially when it appears alongside blood pressure at or above 130/85 mm Hg.[2]
A practical approach: look at your results as a set, not as individual pass/fail grades. Ask your provider not just “are these normal?” but “are these trending in the right direction?”
Advanced Markers: Beyond the Standard Panel
If the standard panel comes back borderline — or if there’s a strong family history — a few additional markers can sharpen the picture considerably.
hs-CRP: The Inflammation Signal
High-sensitivity C-reactive protein (hs-CRP) measures systemic inflammation. Elevated hs-CRP has been shown to independently predict cardiovascular events — not just as a byproduct of metabolic dysfunction, but as a contributor to it.[5]
For metabolic syndrome specifically, chronic low-grade inflammation is thought to both reflect and worsen insulin resistance. An hs-CRP above 3.0 mg/L places someone in the high-risk category for cardiovascular events; values above 1.0 mg/L are worth discussing with a provider when other markers are borderline.
Fasting Insulin and HOMA-IR
Fasting insulin is not part of routine metabolic panels in most US clinical settings — but it’s one of the most informative markers available for catching early insulin resistance. Note that lab reference ranges for fasting insulin vary by laboratory, with many setting “normal” up to 25 µIU/mL. In research contexts, values above 10–15 µIU/mL alongside normal fasting glucose are frequently seen in people years before a prediabetes diagnosis.
HOMA-IR — calculated as fasting glucose (mg/dL) × fasting insulin (µIU/mL) ÷ 405 — is a validated, low-cost way to estimate insulin resistance without more invasive testing. Research generally suggests scores above 2.0–2.5 may indicate elevated resistance, though the precise cut-off varies by population and study. It’s a directional tool, not a diagnostic threshold, and is best interpreted alongside other markers.
Small Dense LDL
Standard lipid panels report total LDL — but LDL particles vary in size and density.
Small dense LDL particles are more readily oxidized and more easily trapped in arterial walls than larger, buoyant LDL particles. This distinction isn’t captured in a standard panel.
An advanced lipid particle test (sometimes called an NMR lipid profile or LDL-P test) can differentiate particle size, though these tests are not widely available in standard clinical settings and may require a referral or out-of-pocket cost. For someone with borderline LDL and multiple metabolic syndrome risk factors, it’s a conversation worth having with a provider.
What These Numbers Tell You — And What to Do Next
Lab results are useful only if they lead somewhere. The research here is more encouraging than most people expect: metabolic markers — even several out-of-range ones — respond well to targeted lifestyle changes, often within weeks to months.
Start with what moves fastest. Triglycerides are one of the most diet-responsive markers in the metabolic panel. Reducing added sugars and refined carbohydrates — even moderately — can lower triglycerides measurably within four to six weeks in many people.
HDL responds more slowly but responds clearly to movement. Adding 20–25 minutes of brisk walking most days of the week supports HDL improvement over an 8–12 week period. Short walks after meals help too — a 10–15 minute walk after the largest meal of the day produces a measurably lower post-meal glucose response than a single longer walk done earlier in the day.[6]
Fasting glucose often shows the most noticeable early shift. Many people see measurable changes in their fasting number within two to four weeks of reducing refined carbohydrate intake, improving sleep, and adding post-meal movement. HbA1c takes three months to move by definition — but the underlying glucose control that will shift it starts improving well before that.
What that might feel like in practice: less pronounced afternoon energy crashes, a more stable morning feeling, fewer cravings in the two hours after a meal. These functional shifts often show up before the next lab draw confirms them.
For more detail on the lifestyle levers with the strongest evidence, the guide on metabolic syndrome lifestyle changes covers what actually moves the needle.
Working With Your Healthcare Provider
Your doctor is interpreting your labs in context — your history, your medications, your family risk. That context is something no online resource can replicate.
A few questions worth bringing to the next appointment:
- Can we add fasting insulin to the next draw?
- What’s the trend on my triglycerides and HDL over the last two years?
- Is an hs-CRP worth checking given my current profile?
- What specific numbers are we targeting — not just “normal” range?
Sharing what you’re actively doing — dietary changes, movement habits, sleep improvements — gives your provider better data to work with. A proactive conversation changes the dynamic from reactive to collaborative.
This cycle of quietly worsening markers can develop over years with no dramatic symptoms — which is why so many people are caught off guard when a doctor first mentions metabolic syndrome. It isn’t a personal failure. It’s a signal the body has been sending for a while, and one that genuinely responds to intervention.
For a broader look at how these markers connect to cardiovascular and hormonal risk, the article on metabolic syndrome signs offers useful context on what to watch for beyond the lab sheet.

Conclusion
Metabolic syndrome blood tests aren’t a verdict — they’re a map. Each marker is a data point, and the pattern across them is what matters most.
The combination of a fasting lipid panel, fasting glucose, fasting insulin (worth requesting specifically), HbA1c, and blood pressure gives a complete enough picture to act on. And these numbers respond — sometimes quickly — to changes that don’t require a prescription.
Understanding what each test measures and why it matters is the first real step. The metabolic syndrome lifestyle changes article on TheMetabolicHub covers what to do once you have that picture.
Frequently Asked Questions
What are the most important metabolic syndrome blood tests to ask for?
The core metabolic syndrome blood tests are a fasting lipid panel (focusing on triglycerides and HDL), fasting glucose, and HbA1c. Adding fasting insulin is worth requesting specifically — it’s not included in most standard panels but gives a much earlier signal of insulin resistance. Blood pressure is also one of the five official diagnostic criteria, though it doesn’t require a blood draw. Together, these measurements provide a complete baseline picture of your metabolic risk.
What is the TG:HDL ratio and why does it matter for metabolic syndrome?
The triglyceride-to-HDL ratio is calculated by dividing your fasting triglyceride level (in mg/dL) by your HDL cholesterol level. A ratio above 3.0 has been associated with insulin resistance in research, even when fasting glucose appears normal — making it a useful early signal that’s already available from a standard lipid panel, no extra test required. A ratio below 2.0 is generally considered favorable from a metabolic health standpoint.
How often should metabolic syndrome blood tests be checked?
For people with borderline markers or established risk factors, annually is a reasonable and commonly recommended schedule. More frequent monitoring — every six months — may make sense if you’re actively working to improve markers through dietary or lifestyle changes, since tracking the trend is as important as any single result. Your provider can help set a monitoring schedule based on your specific profile.
What does borderline mean on a metabolic syndrome lab result?
Borderline numbers are a meaningful signal, not a free pass. They suggest your body is beginning to struggle with one or more metabolic processes — often insulin resistance — and that the overall trajectory is worth addressing. The encouraging part: borderline is also where lifestyle intervention has the strongest evidence for reversing direction, before a pattern becomes entrenched. Think of it as a useful early warning, not a diagnosis.
Can metabolic syndrome blood test results improve with lifestyle changes?
Research consistently supports that metabolic markers respond well to targeted lifestyle interventions. Triglycerides are among the fastest-moving — dietary changes alone can produce measurable reductions within four to six weeks in many people. HDL typically improves over 8–12 weeks with consistent movement. Fasting glucose often shows earlier improvement, with many people noticing changes within two to four weeks of reducing refined carbohydrates and improving sleep quality.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or treatment plan. TheMetabolicHub.com does not replace professional medical guidance.
References
- Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA. 2002;287(3):356–359. PMID: 11790215
- Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. PMID: 16157765
- McLaughlin T, Reaven G, Abbasi F, et al. Is there a simple way to identify insulin-resistant individuals at increased risk of cardiovascular disease? Am J Cardiol. 2005;96(3):399–404. PMID: 16054467
- American Diabetes Association. Standards of Medical Care in Diabetes — 2023. Diabetes Care. 2023;46(Suppl 1). Available at: diabetes.org
- Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. 2000;342(12):836–843. PMID: 10733371
- Buffey AJ, Herring MP, Langley CK, Donnelly AE, Carson BP. The acute effects of interrupting prolonged sitting time with standing and light-intensity walking on biomarkers of cardiometabolic health. Sports Medicine. 2022;52(8):1765–1787. PMID: 35115009
- Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the IDF, NHLBI, AHA, WHF, IAS, and IASO. Circulation. 2009;120(16):1640–1645. PMID: 19805654





